Thrombosis of the mesenteric artery is a violation of blood circulation in the mesenteric vessels. This condition in 25% of cases is the cause of acute intestinal ischemia. Pathology is expressed in severe pain in the lower abdomen, which is accompanied by bloody impurities, as well as shock. To help the patient, he needs to urgently perform an operation.
The superior mesenteric artery supplies blood to the small intestine, caecum, ascending colon, and transverse colon. Part of the transverse colon, all colon, the sigmoid colon, and the rectum are supplied by the inferior mesenteric artery. Most often, the superior mesenteric artery, which is responsible for blood supply, suffers. digestive tract generally. However, a mixed lesion of the mesenteric veins and arteries cannot be ruled out. First, a thrombus clogs the lumen of one vessel, and then a chronic obstruction of another vessel develops. The disease most often affects men over the age of 50 years.
Until now, thrombosis of the mesenteric artery remains an urgent problem for surgeons. This is explained not only by the difficulties in diagnosing a pathological condition, but also by the fact that it can be provoked by many reasons and often leads to the death of the patient.

Thrombosis of the mesenteric artery can be due to several reasons, including:
Postponed operations on the cardiac aorta.
The presence in the body of a tumor of a malignant nature.
Blood hypercoagulability, polycythemia vera, thrombocytosis, sickle cell anemia.
The period of bearing a child.
Reception hormonal drugs for the purpose of contraception.
paraneoplastic syndrome.
Infection of organs located in the peritoneal cavity, including diverticulitis, appendicitis, etc.
Cirrhosis of the liver with portal hypertension leading to venous congestion.
Surgical intervention, accompanied by trauma to the mesenteric artery.
Anastomosis.
decompensated disease.
Thrombosis occurs when the mesenteric artery is blocked by thrombotic masses. As a result, blood flow slows down, which leads to pathological changes in the organ.
There are three options for the development of this pathological condition. In the first case, blood flow can be restored spontaneously, or with the help of medicines(thrombosis with compensation of blood flow of the mesenteric artery). In this case, the functioning of the intestine will not be disturbed.
In the second case, a violation of the blood flow will lead to various diseases of the intestine (thrombosis with subcompensation of the blood flow of the mesenteric artery).
In the third case, a violation of blood flow causes purulent peritonitis, sepsis and death of the patient (decompensated thrombosis).
Elderly people.
Patients with malignant tumors of the peritoneum.
Patients who underwent atrial fibrillation.

Acute thrombosis of the mesenteric artery has a sudden onset. Severe pain comes to the fore. They are localized in the abdomen, proceed according to the type of contractions. A person is not able to stay still, he constantly rushes about in search of a comfortable body position that allows him to relieve pain. The patient feels best when the knees are tightly pressed to the stomach.
Other signs of thrombosis of the mesenteric artery:
The patient is nauseated and may vomit. Bile and blood are found in the vomit. Then the smell of feces will begin to come from vomiting.
The stool is liquid, blood is visible in it.
The skin of the face and body becomes cyanotic.
Shock may develop.
After 6-12 hours from the onset of the development of the pathological process, the pain becomes less intense. At the same time, it acquires a clearer localization, that is, it does not spill over the entire peritoneum, but is concentrated in the intestinal region.
In the area between the navel and the pubis, a tumor-like seal can be felt.
The patient's health is getting worse: the pulse quickens, but arterial pressure comes back to normal.
After 18-36 hours from the start of the first symptoms, the patient develops peritonitis. His condition worsens sharply, the pains become incredibly intense, especially during physical activity. Growing signs of intoxication of the body.
The patient cannot empty the intestines, as its paralytic obstruction develops.
So, in its development, mesenteric artery thrombosis goes through three phases: hyperactive phase (first 6-12 hours), paralytic phase (12-18 hours) and shock (18-36 hours).

During the examination of the patient, who got into medical institution in the first hours from the onset of thrombosis, the doctor will find a soft stomach, the participation of the peritoneal wall in breathing. Symptoms internal irritation the peritoneum is absent, that is, the severity of the pathology does not correspond initial symptoms illness. This is one of the factors complicating the correct diagnosis. An increase in body temperature and signs of irritation of the peritoneum will occur only at the stage of peritonitis, when it will be difficult for the patient to help.
It is imperative to clarify with the patient whether he previously had an attack of angina pectoris with abdominal pain, which would occur after eating. As a rule, about 50% of patients with mesenteric artery thrombosis give a positive answer to this question. Since the process of digestion of food increases intestinal perfusion, the patient may suffer from malnutrition, since such patients often develop fear of eating, and saturation occurs much faster.
Suggestive of thrombosis of the mesenteric artery can be such conditions in the history of the disease as: ischemic heart disease, atherosclerosis, obliterating endarteritis, as well as surgical interventions on the aorta.
What you should pay attention to:
Against the background of the development of intestinal necrosis, the pain may subside somewhat. Patients take this as a trend towards improvement, which is a false opinion.
Narcotic painkillers do not reduce the intensity pain. At the beginning of the development of symptoms of thrombosis, antispasmodics are much more effective.
As the disease progresses, intoxication of the body increases.
Symptoms of thrombosis most often do not correspond to the severity of ischemic bowel disease.
To perform a qualitative diagnosis, it is necessary to perform the following studies:
X-ray of the intestine. Such indicators as: excessive stretching of the intestine, its compacted wall, etc., should pay attention to themselves. The specificity of the method does not exceed 30%.
CT scan of the intestine. Signs of thrombosis of the mesenteric artery: swelling of the intestinal wall, hemorrhages in certain parts of the intestine. This method allows visualization of the thrombus. However, CT with vascular angiography has greater specificity. This study allows to detect thrombosis in 94% of cases.
Angiography of intestinal vessels. Allows you to make a correct diagnosis in 88% of cases.
Ultrasound has specificity in 92-100% of cases. However, if the thrombus is located outside the main vessels, then the study will not allow it to be detected. Therefore, this method is not taken as a basis, regarding it as an auxiliary one.
Other methods to clarify the diagnosis: MRI (disadvantages: expensive research, lack of necessary equipment in many clinics, but the high specificity of the method), echocardiography (makes it possible to clarify the source of a blood clot), ECG, etc.
Blood must be taken from the patient for biochemical and general analysis, as well as for a coagulogram.

After admission to the hospital, the patient is placed in the intensive care unit.
He is shown the following treatment:
Restoration of the water-salt balance of the body.
Correction of the level of electrolytes.
Oxygen therapy.
If there are indications, then the patient is given a blood transfusion.
Pressure and diuresis control.
Placement of a nasogastric tube.
Normalization of the work of the heart muscle.
Relief of pain.
Prescribing broad-spectrum antibacterial drugs.
Use of medicines:
The introduction of Papaverine through a catheter into that part of the intestine that has been affected. The drug is administered throughout the day (this is the minimum period for the supply of the drug). It is impossible to combine the use of Papaverine and Heparin.
The introduction of trobolytics through the catheter, provided that the patient has not yet developed peritonitis or intestinal necrosis. It is important to perform this procedure no later than 8 hours from the onset of symptoms. If after 4 hours the patient does not feel better, then surgery is recommended.
The introduction of Heparin followed by the transition to Warfarin.
Surgical intervention:
Intestinal resection is prescribed provided that the patient develops peritonitis.
Revascularization with further anastomosis can also be considered as a method of surgical treatment for mesenteric artery thrombosis.
According to different authors, the death of patients with mesenteric thrombosis can reach 50-100%. A more accurate prognosis depends on the speed of seeking medical help. It is aggravated by the fact that many patients go to the doctor already developed or with peritonitis. If the patient refuses the operation, then death occurs in 100% of cases.
Prevention of thrombosis of the mesenteric artery
Prevention of thrombosis of the mesenteric artery is reduced to the management healthy lifestyle life, quit smoking. It is also important to monitor body weight, avoiding obesity.
It is imperative to treat all diseases that pose a threat to the formation of a blood clot. We are talking about atherosclerosis, rheumatism, arrhythmias, etc.
Education: Moscow State University of Medicine and Dentistry (1996). In 2003 he received a diploma from the educational and scientific medical center for the administration of the President of the Russian Federation.
thrombotic masses can be removed not only from peripheral arteries, but also from the aortic bifurcation. In severe ischemia accompanied by muscle edema (grade IIIA) or muscle contracture (grade SB), fasciotomy is indicated to decompress and improve tissue blood flow.
In acute thrombosis, which has developed against the background of an organic lesion of the arterial wall, simple thrombectomy is usually ineffective, since rethrombosis of the vessel quickly sets in. Therefore, it should be supplemented with a reconstructive operation. With the development of gangrene of the limb, amputation is indicated.
Forecast. With late diagnosis of acute arterial obstruction and untimely provision of qualified medical care, the prognosis is unfavorable.
18.9.1. Embolism and thrombosis of mesenteric vessels
Acute circulatory disorders in the mesenteric vessels develop as a result of arterial embolism or thrombosis of the mesenteric arteries and veins. The most frequently affected is the superior (90%), less often - the inferior mesenteric artery (10%).
Etiology. The main cause of embolism is heart disease complicated by the formation of blood clots (rheumatic defects, arrhythmias, myocardial infarction, cardiosclerosis, endocarditis). The source of embolism can be atherosclerotic plaques in the aorta, as well as thrombotic masses of the aneurysmal sac. Changes in the vascular wall (atherosclerosis or arteritis) predispose to the occurrence of thrombosis of the mesenteric arteries. The development of thrombosis of the mesenteric veins is possible in the presence of purulent processes in the abdominal cavity (pylephlebitis), portal hypertension, accompanied by stagnation of blood in portal vein, with sepsis, trauma, compression of blood vessels by neoplasms. The disease is equally common in men and women, it develops mainly in middle and old age.
Pathological picture. Due to a violation of the mesenteric circulation, ischemia of the intestinal wall occurs, in which severe destructive-necrotic changes develop, ranging from ischemic to hemorrhagic infarction. With occlusion of a small arterial branch, only a limited area of the intestine suffers, with blockage of the main trunk, all intestinal loops in the area of impaired blood supply die.
Clinical picture and diagnosis. Thrombosis and embolism of the mesenteric vessels have similar clinical symptoms. The disease, as a rule, begins suddenly with an attack of intense abdominal pain, the localization of which depends on the level of vessel occlusion. When the main trunk of the superior mesenteric artery is damaged, pain is localized in the epigastric or umbilical region or spreads throughout the abdomen. With embolism of the iliac-colon artery involved in the blood supply to the terminal ileum and ileocecal angle, pain often occurs in the right iliac region, simulating a picture acute appendicitis. For thrombosis and embolism of the inferior mesenteric artery, the appearance of pain in the left lower quadrant of the abdomen is characteristic. Pain is often constant, sometimes cramping, reminiscent of those with intestinal obstruction. Because of the fear of their strengthening, sick old
lie motionless on their backs, bending their legs at the knee and hip joints.
Nausea and vomiting are observed already in the first hours of the disease in 50% of patients. Subsequently, these symptoms become permanent. Frequent loose stools appear in 20% of patients, often in the feces there is an admixture of unchanged blood. At the onset of the disease, the pulse is usually quickened, the tongue is moist, the abdomen is usually soft, not swollen, and slightly painful.
As the disease progresses, a picture of paralytic ileus develops, characterized by bloating, lack of peristalsis, retention of stools and gases, and frequent vomiting. The tongue becomes dry, the abdomen is painful, muscle tension is noted abdominal wall. On digital examination of the rectum, traces of blood are sometimes found on the glove. The end of the disease is peritonitis.
Acute disorders of the mesenteric circulation are characterized by pronounced leukocytosis (20-30-106/l), which is rare in other acute surgical diseases of the abdominal organs.
X-ray examination of the abdominal cavity provides certain information only in last stage pathological process when there is paralytic ileus. With occlusion of the main trunk of the superior mesenteric artery, X-ray examination reveals swollen loops of the small and right half of the large intestine. At the same time, horizontal levels of fluid are determined in the lumen of the small intestine, which, unlike the levels with mechanical intestinal obstruction, do not move from one knee of the intestine to another.
Patients should undergo latheroscopy, paying attention to changes x-ray picture when turning the torso: inflated intestinal loops in patients with mechanical intestinal obstruction remain fixed when turning the torso from one side to the other; in patients with paralytic ileus of the intestine caused by acute thrombosis or embolism of the mesenteric vessels, they easily move to the overlying parts of the abdomen.
Selective angiography has the greatest diagnostic value. A reliable sign of thrombosis of the mesenteric arteries is the absence of contrast enhancement of the main arterial trunk or its branches on angiograms; vein thrombosis is characterized by the absence of a venous phase and prolongation of the arterial phase. Due to the lengthening of the capillary phase of the study, a longer and more intense contrasting of the intestinal wall is determined.
Differential diagnosis. Acute violation of the mesenteric circulation should be differentiated from acute surgical diseases of the abdominal organs, in particular from mechanical intestinal obstruction, perforated gastric and duodenal ulcers, acute pancreatitis, acute cholecystitis and acute appendicitis. Laparoscopy can be of great help in the differential diagnosis.
Sometimes, a clinical picture similar to acute obstruction of the mesenteric vessels is observed in myocardial infarction with atypical localization of pain. In these cases diagnostic value acquire a carefully collected anamnesis and data of electrocardiographic studies. *&?W
Treatment. Effective only surgery allowing spa
save the life of the patient. In the absence of intestinal necrosis, reconstructive surgery on the mesenteric vessels (embolgectomy, endarterectomy, resection of the superior mesenteric artery with prosthesis or implantation of its stump into the aorta) can be performed. With gangrene of the intestine, its resection is indicated within healthy tissues. In some cases, it is advisable to combine resection with reconstructive surgery on the vessels.
Forecast. Postoperative mortality reaches almost 80%, which is caused not only by the difficulties of diagnosis and the severity of the operation, but also by the presence of the underlying disease, which led to acute mesenteric circulatory disorders.
18.10. Diseases of the small arteries and capillaries
18.10.1. Diabetic angiopathy
It develops in people with diabetes mellitus and is characterized by damage to both small (microangiopathy) and large vessels (macroangiopathy). With microangiopathy, the most significant changes are the vessels of the microvasculature - arterioles, capillaries and venules. Proliferation of the endothelium, thickening of the basement membranes, deposition of mucopolysaccharides in the walls are observed, which ultimately leads to narrowing and obliteration of the lumen. As a result of these changes, microcirculation worsens and tissue hypoxia occurs. The most common manifestations of microangiopathy are diabetic retinopathy and nephropathy.
With macroangiopathy, changes characteristic of atherosclerosis are found in the walls of the main arteries. Against the background of diabetes, favorable conditions are created for the development of atherosclerosis, which affects a younger group of patients and progresses rapidly. Typical for diabetes is Menckeberg's arteriosclerosis - calcification of the middle lining of the artery.
In diabetes, the frequency of multisegmental lesions of the arterial bed is high. Distinctive feature is the defeat of the arteries of medium and small caliber (popliteal, tibial, arteries of the foot).
Diabetic angiopathy of the lower extremities. During angiopathy, there are some specific features: 1) early addition of symptoms of neuropathy with loss of superficial and deep sensitivity and polyneuritis of varying severity (from burning sensation and numbness of individual areas or the entire foot to severe pain syndrome); 2) the appearance of trophic ulcers and even gangrene of the toes with preserved pulsation of the peripheral arteries. Feet infection can occur after minor trauma, cracks, skin necrosis and manifest as cellulitis of the dorsal surface of the foot, deep plantar space abscess, osteomyelitis of the bones of the distal foot, or gangrene of the entire foot; 3) a combination of angiopathy of the lower extremities with retino- and nephropathy.
Clinical picture diabetic angiopathy consists of a combination of symptoms of polyneuropathy, microangiopathy and atherosclerosis of the main arteries. Among the latter, the popliteal artery and its branches are more often affected. Unlike obliterating atherosclerosis, diabetic macroangiopathy of the lower extremities is characterized by a more severe and progressive course, often ending in the development of gangrene.
us. Due to the high susceptibility of patients with diabetes mellitus to infectious diseases, gangrene of the foot is often wet.
The main conditions for the successful treatment of diabetic angiopathy are the optimal compensation of diabetes mellitus and the normalization of the disturbed metabolism of carbohydrates, fats, proteins, and mineral metabolism. This is achieved by the appointment of an individual diet with a restriction of easily digestible carbohydrates and animal fats, anabolic hormones, potassium preparations, hypoglycemic agents (preferably the use of diabetone), as well as adequate therapy with insulin and its analogues. One of the required components complex therapy there must be one or another angioprotector (dobesilate, parmidine, etc.) -
The presence of ulcerative-necrotic changes is not a contraindication to the appointment conservative therapy, which often leads to mummification of limited necrotic areas and their self-rejection. In such cases, preference should be given to intra-arterial infusion of drugs. For patients with severe ischemia of the lower extremities, it is also advisable to carry out gravitational plasmapheresis, which helps to reduce ischemic pain, faster rejection of purulent-necrotic areas and wound healing.
18.10.2. Raynaud's disease
The disease is an angiotrophoneurosis with a predominant lesion of small terminal arteries and arterioles. The disease is observed, as a rule, in young women, accompanied by pronounced microcirculatory disorders. The arteries, arterioles and capillaries of the hands, feet and fingers are affected. The main manifestation of the disease is a recurrent generalized spasm of the arteries listed above, followed by degenerative changes in the walls of the arteries and capillaries, and thrombosis of the terminal arteries. The disease is characterized by spasm of the vessels of the fingers and toes and, very rarely, of the tip of the nose and ears. The process is localized mainly on the upper limbs; the lesion is usually bilateral and symmetrical.
The main causes of the development of Raynaud's disease are prolonged chills, chronic traumatization of the fingers, dysfunction of some endocrine organs(thyroid gland, gonads), severe mental disorders. Disturbances in vascular innervation serve as a "trigger" mechanism in the development of the disease.
There are three stages of the disease.
Stage I - angiospastic. It is characterized by a pronounced increase in vascular tone. There are short-term spasms of the vessels of the terminal phalanges. Fingers (usually II and III) of the hands become deathly pale, cold to the touch and insensitive. After a few minutes, the spasm is replaced by vasodilation. Due to active hyperemia, reddening of the skin occurs and the fingers become warm. Patients note in them severe burning and sharp pain, swelling appears in the area of the interphalangeal joints. When the vascular tone returns to normal, the color of the fingers becomes normal, the pain disappears.
Stage II - angioparalytic. Attacks of blanching ("dead finger") at this stage are rarely repeated, the hand and fingers become bluish in color, and when the hands are lowered down, this coloration intensifies.
and takes on a purple hue. Puffiness and pastosity of the fingers become permanent. The duration of stages 1-11 is on average 3-5 years.
Stage III - trophoparalytic. Panaritiums and ulcers appear on the fingers. Foci of necrosis are formed, capturing the soft tissues of one or two terminal phalanges, less often the finger. With the development of demarcation, rejection of necrotic areas occurs, after which slowly healing ulcers remain, the scars from which are pale in color, painful, soldered to the bone.
Treatment. The use of angiotropic drugs and antispasmodics, physiotherapy, hyperbaric oxygenation are shown. If treatment is ineffective, thoracic or lumbar sympathectomy or stellectomy is performed (depending on the location of the lesion).
18.10.3. Hemorrhagic vasculitis (Schonlein-Henoch disease)
The disease is manifested by small hemorrhages in the skin, mucous membranes and serous membranes. In the mechanism of development of hemorrhagic vasculitis, a toxic-allergic hyperergic reaction to infectious-toxic effects is important ( rheumatic diseases, infections of the upper respiratory tract, beriberi, food poisoning, drug), leading to an increase in the permeability of the capillary endothelium for the liquid part of the blood and formed elements.
Histological examination reveals eosinophilic and neutrophilic cell infiltrates covering the affected vessels in the form of a muff, in places - foci of necrosis. Due to hemorrhages and protein imbibition of the vessel wall, its lumen narrows, local blood flow deteriorates, and focal necrosis occurs.
There are 4 forms of the disease: simple, rheumatoid, abdominal and fulminant. The simple form proceeds with petechial and hemorrhagic rashes. At rheumatoid form there is swelling of the joints. The abdominal form is characterized by cramping pains in the abdomen, resembling acute intestinal obstruction; sometimes there is hematemesis or diarrhea. With a lightning-fast form, hemorrhages are of a confluent nature, often ulcerate. In this regard, hemorrhages appear in the ventricles of the brain, acute ulcers gastrointestinal tract, which may be complicated by perforation. In the kidneys, changes similar to the exudative phase of glomerulonephritis can be detected, in the lungs - foci of pneumonia with a hemorrhagic component.
Treatment. The basis of treatment is anti-inflammatory and desensitizing therapy, the use of steroid hormones. Surgery is indicated for intra-abdominal complications.
Chapter 19
There are superficial and deep veins of the extremities.
Superficial veins of the lower extremities represented by the great and small saphenous veins. The great saphenous vein (v. saphena magna) starts from the internal marginal vein of the foot, is located in the depression between the anterior edge of the medial malleolus and the tendons of the flexor muscles, and rises along the inner surface of the lower leg and thigh to the oval fossa.
where at the level of the lower horn of the falciform margin of the wide fascia of the thigh flows into the femoral vein. The external pudendal veins (vv.pudendae externae), the superficial epigastric vein (v.epigastrica superficialis) flow into its uppermost segment, superficial vein surrounding under the ilium (v.circurnflexa ileum superficialis). Distal to 0.5-2.5 cm, two larger accessory veins flow into it - w.saphena accessoria medialis and saphena accessoria lateralis. These two tributaries are often well defined and have the same diameter as the main trunk of the great saphenous vein. The small saphenous vein (v.saphena parva) is a continuation of the lateral marginal vein of the foot, begins in the depression between the lateral ankle and the edge of the Achilles tendon and rises along the posterior surface of the lower leg to the popliteal fossa, where it flows into the popliteal vein. There are many anastomoses between the small and large saphenous veins on the lower leg.
Deep venous network of the lower extremities It is represented by paired veins that accompany the arteries of the fingers, foot, and lower leg. The anterior and posterior tibial veins form an unpaired popliteal vein, which passes into the trunk of the femoral vein. One of the major tributaries of the latter is the deep vein of the thigh. At the bottom edge inguinal ligament the femoral vein passes into the external iliac vein, which, merging with the internal iliac vein, gives rise to the common iliac vein. The latter merge, forming the inferior vena cava.
Communication between the superficial and deep venous system is carried out by communicating (perforating or perforating) veins. There are direct and indirect communicating veins. The first of them directly connect the saphenous veins with the deep ones, the second carry out this connection through the small venous trunks of the muscular veins. Direct communicating veins are located mainly along the medial surface of the lower third of the leg (Cockett's group of veins), where there are no muscles, as well as along the medial surface of the thigh (Dodd's group) and lower leg (Boyd's group). Usually the diameter of the perforating veins does not exceed I-2 mm. They are equipped with valves that normally direct blood flow from superficial veins to deep veins. With valve insufficiency, there is an abnormal flow of blood from the deep veins into the superficial ones.
The superficial veins of the upper limb include the saphenous venous network of the hand, the medial saphenous vein (v.basilica) and the lateral saphenous vein of the arm (v.cephalica). V.basilica, being a continuation of the veins of the rear of the hand, rises along the medial surface of the forearm, shoulder and flows into the brachial vein (v.brachialis). V.cephalica is located on the lateral edge of the forearm, shoulder and flows into the axillary vein (v.axillaris).
Deep veins are represented by paired veins accompanying the arteries of the same name. The radial and ulnar veins drain into two brachial veins, which in turn form the trunk of the axillary vein. The latter continues into the subclavian vein, which, merging with the internal jugular vein, forms the brachiocephalic vein (v.brachicephalica). From the confluence of the brachiocephalic veins, the trunk of the superior vena cava is formed.
The veins of the lower extremities have valves that promote the movement of blood in a centripetal direction and prevent its reverse flow. The ostial valve is located at the confluence of the great saphenous vein with the femoral vein, which restrains the reverse flow of blood from the femoral vein. There are a significant number of such valves throughout the great saphenous and deep veins. Promotion of blood in the centripetal direction is facilitated by the difference between the relatively high pressure in the peripheral veins and the low pressure in the inferior vena cava. The systolic-diastolic oscillations of the arteries, which are transmitted to the adjacent veins, and the “sucking” action of the respiratory movements of the diaphragm, which lowers the pressure in the inferior vena cava during inspiration, also contribute to the movement of blood in the centripetal direction. An important role also belongs to the tone of the venous wall.
An important role in the implementation of the return of venous blood to the heart is played by the muscular-venous pump of the lower leg. Its components are venous sinuses of the calf muscles (sural veins), in which a significant amount of venous blood is deposited, calf muscles, squeezing with each contraction and pushing venous blood into deep veins venous valves, preventing backflow of blood. The essence of the mechanism of action of the venous pump is as follows. At the moment of relaxation of the muscles of the lower leg ("diastole"), the sinuses of the soleus muscle are filled with blood coming from the periphery and from the superficial venous system through the perforating veins. With each step, the calf muscles contract, which compresses the muscular venous sinuses and veins ("systole"), directing blood flow into the deep main veins, which have a large number of valves throughout. Under the influence of increasing venous pressure, the valves open, directing blood flow into the inferior vena cava. Downstream valves close to prevent backflow.
The blood pressure in a vein depends on the height of the hydrostatic (distance from the right atrium to the foot) and hydraulic blood pressure (equivalent to the gravitational component). V vertical position body, the hydrostatic pressure in the veins of the legs and feet increases sharply and is added to the lower hydraulic pressure. Normally, venous valves restrain the hydrostatic pressure of the blood column and prevent vein overstretching.
From this article you will learn: the causes and symptoms of mesenteric thrombosis, why it is dangerous. Methods of prevention and treatment.
Article publication date: 05/15/2017
Article last updated: 05/29/2019
Thrombosis of the mesenteric vessels is a blockage of the vessels of the mesentery (mesenteric) by a thrombus. The mesenterium is a collection of mesenteric cords, with the help of which the abdominal organs are attached to the abdominal wall. This is a very dangerous condition.
The arteries and veins passing through the mesenterium are responsible for the blood circulation of the abdominal organs, primarily the intestines. And if a thrombus occludes a mesenteric artery or vein, it will lead to serious violations bowel movements and, if left untreated, to death.
Mesenteric thrombosis is treated with surgery. The treatment is carried out by a surgeon.
The disease is accompanied by a very high mortality due to its transience and difficulties in diagnosis.
Causes
Mesenteric thrombosis, like any other, is directly related to cardiovascular and blood diseases. Thrombi are formed in heart failure, inflammatory processes in the vessels, after myocardial infarction, arrhythmias, cardiosclerosis, aneurysms of the heart walls and blood vessels, inflammation of the heart.
The risk of thrombosis increases with:
- thrombophilia (hereditary predisposition to the formation of blood clots);
- surgical operations and injuries;
- long-term use of drugs that increase the "viscosity" of the blood (anticancer drugs, oral contraceptives);
- prolonged immobilization of the body (in bedridden patients or disabled people on a wheelchair, while lying in the postoperative period);
- pregnancy and postpartum period;
- diabetes;
- obesity
- smoking.
Regardless of where a thrombus has formed, it can block any artery or vein, including the mesenteric one.
The risk that a thrombus will clog the mesenteric vessel increases with severe infectious diseases intestine and its tumors.
 Vessel in section, on an enlarged scale. The process of thrombus formation in atherosclerosis
Vessel in section, on an enlarged scale. The process of thrombus formation in atherosclerosis Symptoms and stages
The disease proceeds in three stages:
- Ischemia. When the vessel lumen is narrowed by 70% or more due to a thrombus, a lack of blood circulation in the intestine develops.
- Intestinal infarction - the death of the area of \u200b\u200bthe intestine that was supplied with blood by the affected vessel.
- Peritonitis - inflammation of the peritoneum, an increase in intoxication of the body. This stage can be fatal.
Symptoms thrombosis of the mesenteric vessels of the intestine:
Thrombosis can proceed very quickly, so when the first symptoms appear, call an ambulance, because the patient needs emergency operation. Symptoms characteristic of stage 1 may also indicate appendicitis, as well as acute gynecological diseases. They also require urgent surgery.

Diagnostics
It is very important to distinguish mesenteric thrombosis from other bowel diseases (appendicitis, perforated ulcer duodenum), as well as from gynecological diseases (for example, ectopic pregnancy ruptured ovarian cyst).
In the presence of the symptoms described in the previous section of the article, the ambulance delivers the patient to the surgical department.
The surgeon makes the diagnosis. It includes the collection of anamnesis and those present at the this moment symptoms, manual examination of the patient. Further, a blood test, a coagulogram (blood clotting test), a urinalysis, an abdominal ultrasound, an emergency angiography of the abdominal vessels are prescribed.
If the diagnosis has not been established, they resort to laparoscopy - an invasive diagnostic method. The organs of the abdominal cavity are examined using an endoscope inserted through an incision in the skin and anterior abdominal wall. The procedure is carried out under anesthesia.
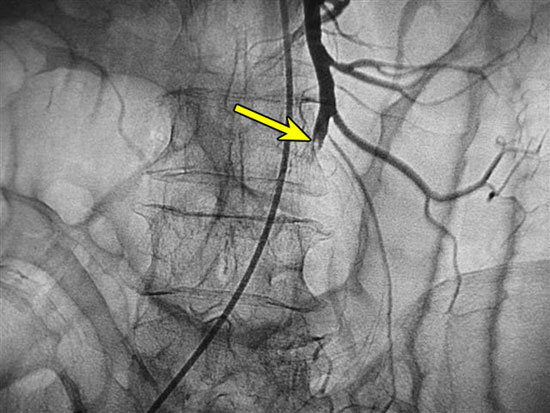 Angiography of the vessels of the abdominal cavity. The arrow indicates the site of thrombosis of the inferior mesenteric artery.
Angiography of the vessels of the abdominal cavity. The arrow indicates the site of thrombosis of the inferior mesenteric artery. Treatment and prognosis
Mesenteric intestinal thrombosis is treated with emergency surgery.
It is carried out in several stages:
- First, the thrombus that provoked circulatory disorders is removed.
- Then the affected vessel is reconstructed.
- If the operation is performed not at stage 1, but at stage 2 of the disease, and the zone of intestinal infarction is extensive, then the dead part of the organ is removed. At stage 3, if a strong inflammatory process has developed, the abdominal cavity is washed.
The outcome of the disease depends on the stage at which it was identified and treated, as well as on the correctness of the diagnosis.
At stages 2 and 3 of the disease with intestinal infarction, even with a successful operation, about 70% of patients die. This may be due to intoxication of the body from the inflammatory process, the severity of the operation, as well as the underlying disease that caused thrombosis. At stage 1 of the disease, if the thrombus is removed before the necrosis of the intestinal area, the survival rate is much higher.
Therefore, do not delay contacting a doctor if you experience abdominal pain.
 Surgery to remove the necrotic part of the intestine. Anastamosis - a special connection of "sections of the chain"
Surgery to remove the necrotic part of the intestine. Anastamosis - a special connection of "sections of the chain" Prevention
It is better to prevent mesenteric thrombosis than to treat it later. With the help of preventive measures, you can literally save your life.
If you suffer from cardiovascular diseases, or your direct relatives were prone to blood clots, pay special attention.
- First of all, exclude all other risk factors (excess weight, smoking, sedentary lifestyle, taking oral contraceptives). Treat diseases of the heart and blood vessels in time. If you have diabetes, follow all the doctor's recommendations regarding treatment.
- If you are at risk of blood clots (suffer from cardiovascular diseases, diabetes, lead a sedentary lifestyle for health reasons, have excess weight associated with metabolic disorders that you cannot get rid of at the moment), then donate blood every six months on a coagulogram. This is necessary to detect bleeding disorders. If you have an increased risk of blood clots, you may be prescribed blood thinners to prevent blood clots from forming.
- Treat bowel disease promptly. If you have a tumor, do not delay its removal. In the case of taking a course of anticancer drugs, periodically take a blood test for clotting and take antiplatelet agents or anticoagulants prescribed by your doctor.
- If you have undergone surgery on the abdominal organs, follow all the doctor's recommendations in the postoperative period. After a blood test, if indicated, the attending surgeon may prescribe you medication to prevent blood clots. Start moving as soon as possible. Walk more if your doctor allows you to. Activity will help prevent not only blood stasis (which increases the risk of blood clots), but also the formation of postoperative adhesions, which can lead to complications in the future.
- After any operations on the vessels (not only on the vessels of the abdominal cavity) and on the heart, take anticoagulants or antiaggregants prescribed by your doctor.
Folk remedies for the prevention of thrombosis
Do not try to replace medicines with folk remedies, as the lack of medical treatment prescribed by a doctor can lead to the formation of blood clots and serious consequences. Also folk remedies may have contraindications, so before taking, consult with a general practitioner, cardiologist and gastroenterologist.
| Components | How to cook | How to use |
|---|---|---|
| Black elderberry (flowers) Air (roots) Cornflower (flowers) horsetail Elecampane (roots) Wild strawberry (leaves) Lovage (leaves) Horse chestnut (flowers) Lilac (leaves) viburnum leaves walnut leaves Plantain (leaves) |
Take 1 g of each plant. Pour 450 ml of water at room temperature. Let it brew for 6 hours. Put on fire, heat to 100 degrees (to a boil) and immediately remove. Put in heat. Wait an hour. Strain. |
Dosage: 1/3-1/2 cup depending on weight. Receptions per day - 3. Reception time - 20 minutes after eating. |
| succession Calamus roots Mother and stepmother (sheets) Tatarnik (flowers) strawberry leaves Mullein flowers horse chestnut flowers birch leaves pepper mountaineer Motherwort |
Take 1 g of each indicated component. Pour in 420 ml of boiling water. Prepare a water bath. Put the decoction on it and keep it for 15 minutes. Remove from the water bath and place in a warm place. Let it brew for 120 minutes. Strain. |
Dosage - 1/3 cup. The number of receptions per day - 3-4 Reception time - 20 minutes after the meal. |
Take these medicinal preparations under the supervision of your physician.
Acute disorders of blood flow in the mesenteric vessels are serious and deadly diseases that require urgent surgical care. Intestinal thrombosis, which manifests itself in successive stages from ischemia to infarction and peritonitis, can cause severe pain and death in the absence of a timely operation: the prognosis for life is favorable with a timely diagnosis.
mesenteric infarction
Acute disturbance of blood circulation in the vessels supplying the intestinal wall leads to local tissue ischemia. In the absence of medical care, intestinal thrombosis causes wall necrosis: the contents of the gastrointestinal tract enter the abdominal cavity, forming severe form surgical pathology - peritonitis.
Most often, mesenteric intestinal thrombosis occurs in the elderly, but it is quite possible that signs acute abdomen in relatively young people against the background of the pathology of the coagulation system or with cardiac diseases.
To understand what the intestines are and what is the danger to life and health, it is necessary to know the characteristics of blood flow and the main causes of pathological blockage of blood vessels.
Features of the blood supply to the intestines
The main supply of the intestine with blood saturated with oxygen and nutrients, and venous outflow is carried out through the following vascular trunks:
- superior and inferior mesenteric arteries;
- paired mesenteric veins - superior and inferior.
Important features of blood flow are:
- the superior mesenteric artery departs from the aorta at an acute angle, which dramatically increases the risk for blockage (this is a kind of trap for emboli and blood clots);
- a large area of responsibility (the upper artery supplies the entire small and part of the large intestine);
- a gradual decrease in the lumen of the vessel from 9-12 mm in the region of the mouth to 4-5 mm in the region of the mesentery;
- impossibility of compensatory blood flow from the inferior to the superior mesenteric artery;
- an insufficient number of venous vessels that ensure the discharge of blood into the vena cava, therefore, venous mesenteric thrombosis is a dangerous type of pathology.
The anatomical features of the vessels in the intestinal region increase the risk of acute and deadly conditions associated with occlusion of the main blood trunks.
Intestinal circulatory system
Causes of ischemic disorders
Circulatory problems in the arteries and veins that feed the intestinal wall are in most cases due to diseases of cardio-vascular system. The main causes of thrombosis of mesenteric vessels:
- atherosclerotic disease;
- myocardial infarction (we wrote more about this disease);
- any type of heart disease;
- pathology of the aorta, congenital or acquired;
- arterial hypertension;
- vascular inflammation (, thromboangiitis, periarteritis);
- varicose disease;
- traumatic injuries of the abdomen;
- tumor-like formations of internal organs;
- thrombophilia (congenital tendency to thrombosis);
- allergic or medicinal angiospasm.
A large number of factors that provoke or create conditions for thrombosis of mesenteric vessels, and the rapid development of local necrotic changes form a negative prognosis of the disease: acute arterial thrombosis of the intestine and peritonitis dramatically worsen a person's chances of survival.
Classification of mesenteric thrombosis
Depending on the cause of mesenteric thrombosis, the following options for blockage of vessels in the intestine are distinguished:
- embolism of the arterial trunks of the mesentery;
- thrombosis of the mesenteric artery;
- mesenteric vein thrombosis;
- pathology of the aorta (thrombus, aneurysm, dissection), resulting in thrombosis of the mesenteric vessels;
- mechanical compression by the tumor;
- surgical ligation of tissues.
An important prognostic factor is the state of blood circulation in the vascular system of the intestine.. Thrombosis of mesenteric vessels can be in the stage of:
- Compensation (clinical manifestations are minimal, the prognosis is favorable);
- Subcompensation (increasing negative symptoms);
- Decompensation (severe condition, poor prognosis).
Be sure to take into account the severity of vascular disorders. Thrombosis of the intestinal vessels leads to the following successive stages of the pathological process:
- Ischemic changes;
- Infarction of the intestinal wall;
- Peritonitis against the background of necrosis of the intestine.
One of the frequent factors of thrombosis of mesenteric vessels are cardiac diseases.
Against the background of congenital anomalies and acquired valvular defects, it is necessary to carry out preventive treatment, especially during the preparation phase and after heart surgery.

Symptoms of pathology
Acute mesenteric thrombosis provides the most striking clinical manifestations, when the following symptoms are typical:
- severe unbearable pain in the abdomen, lasting several hours;
- forced posture (legs pulled up to the stomach);
- extreme anxiety and fear, moans and cries;
- and increased blood pressure;
- great pallor and cold sweat;
- vomiting and loose stools.
Usually, such a bright clinic occurs when thrombosis of the superior mesenteric artery occurs. The ischemic stage ends, and after 6-12 hours from the onset of pain, a temporary improvement occurs. The stage of intestinal infarction is characterized by significant relief, up to the cessation of the pain syndrome. Vascular pressure may return to normal, but the heart rate does not decrease. At this stage, mesenteric intestinal thrombosis is manifested by blood in the stool and vomit, increasing signs of intoxication.
With the onset of peritonitis, which is characterized by the resumption of severe pain, the chances of recovery are sharply reduced. The most important factors that ensure favorable prognosis are timely diagnosis and surgical treatment of the disease.
Diagnostic methods
At the initial surgical examination, performed by an experienced specialist, it is possible to quickly assume the presence of an acute abdomen. In addition to conducting the necessary palpation tests, the doctor will refer you to the following examinations:
- determination of the number of leukocytes in a general clinical blood test;
- assessment of blood coagulation by coagulogram;
- ultrasound scanning of internal organs;
- plain x-ray of the abdomen;
- CT scan;
- angiographic examination to determine the site of blockage;
- diagnostic laparoscopy.
Depending on the symptoms and severity, the examination tactics are individual. Everything diagnostic measures must be performed quickly to prevent deterioration and progression of the disease: thrombosis of the mesenteric vessels in the compensation stage can be cured without dangerous consequences, and against the background of peritonitis, the risk of death increases to 90%.

Tactics of surgical treatment
Progressive mesenteric thrombosis, which requires urgent treatment, cannot be eliminated medicines. The only chance to save a life is a surgical operation, the main goals of which are:
- Restoration of blood flow;
- Removal of the necrotic part of the intestine;
- Fight inflammation in the abdominal cavity.
The main stages of surgical intervention:
- Incision of the abdominal wall for access to internal organs;
- Assessment of the state of the intestine (viability of the wall, detection of foci of tissue necrosis)
- Determination of vascular pulsation and palpation finding the place where mesenteric intestinal thrombosis occurred;
- Removal of a non-viable part of the intestine (resection);
- Imposition of an anastomosis to restore intestinal patency;
- Carrying out activities for the sanitation of the abdomen to prevent peritonitis after surgery.
Drug therapy in the postoperative period is necessary to prevent complications and prevent recurrent thrombosis.
A large role in the restoration of bowel function is given to rational diet therapy: it is necessary to carefully and clearly follow the doctor's recommendations on nutrition.
Complications and consequences
Sudden thrombosis of the mesenteric vessels leads to the following dangerous conditions and diseases:
- acute abdomen with severe pain;
- necrosis of the intestinal wall with perforation and peritonitis;
- sepsis as one of the causes of death;
- the formation of a purulent abscess of the abdominal cavity;
- expressed adhesive process as an outcome of inflammation;
- short bowel syndrome with unpleasant symptoms;
- intestinal dysbiosis.
Most of pathological conditions extremely negatively affects human health, reducing the quality of life and increasing the risk of recurrent thrombosis in any vessels of the body.
Forecast for life
Acute thrombosis of the mesenteric arteries without surgical treatment ends in the death of a person (up to 75% of people die in the first 2-3 days from the onset of the pain syndrome). With venous blockage, the time of death is delayed by a couple of days (by 4-5 days). When conducting surgical operation to the maximum early term the chances of survival increase dramatically (two-thirds of patients operated on the first day recover). V remote period it is necessary to continue monitoring with a vascular surgeon and a cardiologist with the obligatory prophylactic administration of drugs that reduce the risk of thrombosis.
It is known that thrombosis is extremely dangerous disease, and with some of its types, the expense of saving the patient's life goes literally for minutes. For example, thrombosis of mesenteric veins and arteries, mortality from this disease is high, only surgery can help. To a greater extent, the elderly suffer from mesothrombosis, due to pathological changes in the vessels. Mesenteric thrombosis begins to develop when there is a violation of blood supply in the vessels of the mesentery (a fold in the peritoneum, due to which the intestine is located vertically), some experts call this pathology an intestinal infarction. But if heart attack has pronounced symptoms, then mesothrombosis is diagnosed problematic and rarely on initial stages which is why the mortality from this disease is so high. To increase the chance of a successful recovery, it is necessary to be informed about the causes of intestinal thrombosis, to know its symptoms.
Development features
Recall that our intestines are supplied with blood by two large vessels - the upper and lower mesenteric (mesenteric) arteries, the first of these arteries mainly feeds the small intestine, the second - the rectum. If the upper part during the development of various diseases can take on the functions inferior artery and feed the colon, the inferior mesenteric artery cannot do the work of the superior mesenteric vein. Therefore, with thrombosis of the mesenteric artery, there is a violation of the blood supply in the small intestine, which leads to the death of the patient. When one of the vessels is blocked, a certain section of the small intestine begins to die, over time, necrosis only spreads.
In 9 out of 10 cases, thrombosis of the superior mesenteric artery develops, which supplies blood to almost the entire intestinal tract, with this pathology it is already difficult to save a person.
However, this type of thrombosis is extremely rarely diagnosed in people under 50 years of age, because with age, atherosclerotic plaques more and more adhere to the walls of the intestinal vessels, which leads to a narrowing of the lumen in the artery. Mortality from this disease is extremely high, and even surgical intervention does not guarantee that necrosis will stop spreading to other tissue areas.
Etiology of the disease
Usually mesenteric thrombosis is a consequence of other diseases that lead to the formation of cholesterol plaques or their rupture. The main reasons are as follows:
- vascular atherosclerosis - with this disease, there is an accumulation of atherosclerotic plaques on the walls of blood vessels, as a result of which thrombosis develops;
- hypertension - high blood pressure contributes to the rupture of cholesterol plaques;
- myocardial infarction is also a consequence of the formation of blood clots;
- endocarditis - with this heart disease, blood clots form;
- thrombophlebitis - in this case, blood stagnation occurs in the veins, which leads to the formation of blood clots;
- rheumatism - with the development of this disease, heart defects are possible, which causes the formation of blood clots;
- postoperative period;
- thrombosis after childbirth;
- sepsis.
Also, thrombosis of the intestinal arteries can cause severe injuries of the abdominal cavity, malignant tumors, various liver diseases. As you can see, the causes of mesothrombosis can be different, but what they have in common is thrombosis.
Symptoms
Often, thrombosis of arteries in the intestine begins with acute stage. As mentioned above, this disease is dangerous because there are no pronounced symptoms in the primary stages of mesenteric thrombosis. A month after the onset of the disease, the patient may experience sharp pains in the area of the peritoneum. The patient may also be concerned about:
- flatulence;
- belching;
- vomit;
- diarrhea;
- severe pain immediately after eating.
All symptoms occur due to narrowing of the lumen in the intestinal vessel. Arterial thrombosis develops rapidly, it takes just a couple of days.
At the most early stages patients may experience subfebrile temperature or mild abdominal pain that long time are not localized.
In the ischemic form, thrombosis of the intestinal vessels is characterized by a very severe pain. The patient often screams from unbearable pain, in agony people cannot find a place for themselves. Moreover, the pain is practically not removed by anything, even strong painkillers.
The following pronounced symptoms are noted:
- skin is pale, almost white;
- the pulse is weakly palpable;
- there is a sharp rise in blood pressure.
On palpation, the abdomen is soft. There is always an increased number of leukocytes in the blood, which indicates an inflammatory process. The pain may be localized in the epigastrium, and may be throughout the peritoneum. Almost all patients begin severe vomiting, in one part diarrhea is observed, and in the other, on the contrary, stool retention.
The ischemic stage develops in about 12 hours, followed by intestinal infarction, which can last up to 24 hours. During this period, the pain subsides somewhat, this is due to necrosis of the intestinal tissues. Patients stop suffering from pain, but due to severe intoxication of the body, their actions become inadequate, sometimes incoherent speech is observed. The pressure normalizes, the pulse is restored, but the level of leukocytes in the blood continues to increase. And the pain is already concentrated at the site of damage to the intestinal vessels.
Without timely surgical intervention, peritonitis occurs in 20-36 hours. Pain again begin to intensify, with palpation of the abdominal cavity, the pain is unbearable, sudden movements also become painful.
The general condition of the patient deteriorates sharply, this is affected by the violation of the electrolyte balance in the body, the rapid spread of necrosis in the tissues, and dehydration of the body.
In the stage of peritonitis, there is very high level white blood cells, the skin is gray, the tongue becomes dry, the pulse is practically not palpable, the blood pressure is high.
If thrombosis of the mesenteric vessels was diagnosed late and timely surgical intervention was not carried out, then after two days of the development of the disease, a person dies from severe intoxication of the body and intestinal peritonitis.
Diagnostics
To make an accurate diagnosis of mesothrombosis, specialists use the following types of diagnostics:
- complete blood count (with this disease, there is always a high level of leukocytes in the blood and ESR);
- with the help of a contrast agent, angiography of the vessels in the intestine is performed, thanks to this study, it is possible to determine the location of the blockage of the artery;
- laparoscopy is performed to assess the condition of the intestinal walls;
- if laparoscopy is not possible, then a laparotomy is performed. When an intestinal infarction is detected, necrotic tissue in the affected area of the intestine is usually removed immediately.
Treatment Methods
At the first signs of thrombosis of the mesenteric vessels of the intestine, it is necessary to immediately call an ambulance, or take the person to the hospital on your own, because the bill often goes on for minutes. Before transportation, you can give the patient heart drops, such as Corvalol or Valocardin. Everything further treatment produced exclusively in stationary conditions. Depending on the stage of the disease, the doctor prescribes therapy.
If intestinal thrombosis is diagnosed, treatment often begins with taking anticoagulants, which improve blood flow and help dissolve the thrombus (Heparin or its analogues). Antithrombotics are also administered intravenously, with the onset of timely drug therapy, it is possible to achieve the dissolution of the thrombus and prevent serious consequences.
But unfortunately, early diagnosis practically impossible, due to the unexpressed symptoms of mesothrombosis during the initial development of the disease.
Therefore, usually specialists resort to surgical intervention, most often this is the only chance for a patient to have a successful outcome.
Despite the fact that in most cases the operation is performed urgently, there is still a preparatory period, a thorough bowel lavage is performed, and medical preparation.
To remove a thrombus or resect a dead tissue site, a laparotomy is performed, often the thrombus has to be literally squeezed out of the vein with your fingers. Instead of the removed part of the vessel, an artificial prosthesis is placed. If necrosis has developed in the tissues, then part of the intestine is removed, and then shunting or angioplasty takes place. If normal blood flow is not restored in a short time, then the patient dies right on the operating table. Postoperative period passes in a hospital within 3 weeks.
Now you know what mesenteric intestinal thrombosis is - this is an extremely dangerous disease, in most cases leading to death. But serious consequences can be avoided if mesothrombosis is diagnosed in time.
In contact with
Offer from Sberbank
Where will payments be made to bank yugra depositors
Business loan without collateral and guarantors
Application form for a home loan from Sberbank
Sberbank AST - electronic trading platform