The main properties of the Conjunctiva are structure tenderness, pale pink color, transparency and surface moisture (color picture 4). There are several divisions of the Conjunctiva. The part of it that covers the posterior surface of the eyelids is called the conjunctiva of the eyelids (conjunctiva palpebrarum); the part covering the sclera is the conjunctiva of the eyeball or sclera (conjunctiva bulbis. sclerae), and the places of transition from the upper and lower eyelids to the eyeball are the upper and lower fornix of the conjunctiva (fornix conjunctivae sup. et inf.). The slit-like capillary space, limited in front by the eyelids, and behind by the anterior part of the eyeball, is called the conjunctival sac. The conjunctiva of the eyelids is subdivided into the conjunctiva of the cartilage (conjunctiva tarsi) and the orbital conjunctiva (conjunctiva oxbitalis), or the transitional fold, which covers the posterior surface of the eyelid from the edge of the cartilage to the arch. It is called a fold because here the conjunctiva with open eyelids forms horizontal folds, which allows the eyeball to maintain its mobility. The upper arch is deeper than the lower one.
The conjunctiva of the cartilage at the free edge of the eyelid has a smooth surface, but already 2-3 millimeters above (in the lower eyelid - below) the free edge, the surface becomes slightly rough. At the outer corner of the eyelid (the corners of the cartilage), the roughness is noticeable with the naked eye, but in the rest of the length it can be detected with a magnifying glass. Roughness is due to the presence of papillae. Normally, through the transparent conjunctiva of the cartilage, the glands of the cartilage of the eyelids (meibomian glands) shine through in the form of thin yellowish lines, parallel to each other. The conjunctiva of the eyeball is very delicate, it is smooth, transparent, the white color of the sclera shines through it. Only at the limbus the conjunctiva is closely soldered to the underlying tissues. The conjunctiva, loosely connected to the eyeball, moves freely and swells during inflammatory processes. At the limbus, patches of pigmentation are sometimes visible.
In the inner corner of the eye, the conjunctiva participates in the formation of the lacrimal caruncle (caruncula lacrimalis) and the lunate fold (plica semilunaris conjunctivae). The lacrimal meat is similar in structure to the skin (only the stratum corneum is absent), contains small hairs, sebaceous and acinous glands. Somewhat outward from it there is a semilunar fold formed by the conjunctiva of the sclera; it is a vestigial organ corresponding to the third century in animals and consists of stratified epithelium and connective tissue.
Histologically, the conjunctiva distinguishes between the epithelium layer (epithelium conjunctivae) and the connective tissue base - the proper lamina of the Conjunctiva (lamina propria conjunctivae).
Epithelium of the conjunctiva of the eyelids is multilayer (color picture 1), its surface layer consists of cylindrical cells, deep - of cubic cells; in the conjunctiva covering the cartilage of the eyelids, 2-4 layers of cells, in the transitional fold - up to 5-6. In the epithelium there are many mucous (goblet) cells that secrete mucous contents - mucin. There are more goblet cells on the conjunctiva of the lower eyelid than on the upper eyelid (color picture 2). On the conjunctiva of the eyeball, the multilayer epithelium changes its character: the surface layer becomes flat, and near the limbus of the cornea it becomes multilayered flat and without a sharp border passes into the corneal epithelium. There are very few mucous cells in the epithelium of the conjunctiva of the eyeball.
The tarsal part of the Conjunctiva (color picture 3) is tightly welded to the cartilage of the eyelid, between them there is a relatively thin layer of the connective tissue base. The orbital part of the conjunctiva of the eyelids, as well as the conjunctiva of the eyeball, is connected to the underlying tissue of the loose-subconjunctival base (tela subconjunctivalis), which facilitates the mobility of both the conjunctiva and the eyeball itself.
Connective tissue base The conjunctiva of the eyelids can be divided into two layers, differing in the distribution and nature of cells and fibers: subepithelial (adenoid) and deep (fibrous).
The subepithelial layer of the Conjunctiva is formed in general from the same two basic elements as the true lymphoid tissue - from the reticular stroma (reticulum), plasma cells and lymphocytes, sometimes forming small clusters - follicles. The deep layer is represented by loose fibrous connective tissue, relatively poor in blood vessels and cellular elements.
In the normal conjunctiva of an adult, there is an abundance of poorly differentiated cells and various histiocytic elements. In the subepithelial layer there is a network of argyrophilic fibers, in the loops of which cells accumulate. Elastic thin filaments are presented in a small amount (Figure 1).
In the first 2-3 months of human extrauterine development, the connective tissue base of the eyelid conjunctiva (its own lamina) consists of loose connective tissue and thin collagen fibers (Figure 2). In it, in contrast to the conjunctiva of adults, a significantly smaller number of cellular elements and a greater tenderness and looseness of the location of the fibers of the connective tissue base are found.
The composition of the cells of the lamina propria of the Neonatal Conjunctiva is also significantly different from that of the Adult. Lymphocytes are rare in comparison with other cells, mainly in the surface layer, near the blood vessels. Plasma cells are completely absent. The bulk of the cells of the lamina propria of the neonatal conjunctiva are fibroblasts and cambial elements.
The changes observed in the conjunctiva in the elderly are characterized by a decrease in the number and change in the composition of cellular elements, as well as an increase in the collagenization process, which leads to a decrease in the number of argyrophilic fibers. Together with the relative depletion of the subepithelial layer of cellular elements, the number of poorly differentiated forms and lymphocytes decreases. Plasma cells, which often show signs of dystrophy, become the main elements of infiltration of the subepithelial layer. Collagen bundles become thicker, coarser, and often undergo hyalinosis. Subepithelial tissue in the elderly loses its adenoid structure (Figure 3).
The glands of the Conjunctiva (Krause's glands), located in the upper and lower transitional fold, are similar in structure and nature of the secretion to the lacrimal gland. They number from 20 to 30 in the upper eyelid and only 6-8 in the lower. For the most part, they are round or oval in shape and are located in the subepithelial layer. Each gland consists of a number of lobules and has a common excretory duct. The same glands (Waldeyer's glands) are found on the border of the tarsal and orbital parts of the Conjunctiva. In the temporal part of the upper fornix of the Conjunctiva, the excretory ducts of the lacrimal gland open.
 |
 |  |
Rice. 1-3. Micropreparations of the conjunctiva (norm): Figure 1 - limbal conjunctiva (the arrow indicates the stratified squamous epithelium); Figure 2 - conjunctiva of the transitional fold (arrows indicate goblet cells in stratified columnar epithelium); Figure 3 - the conjunctiva of the eyelid cartilage (the arrow indicates the stratified columnar epithelium). |
||
The conjunctiva is abundantly vascularized. Its vascularization involves the posterior conjunctival vessels emanating from the system of arterial arches of the upper and lower eyelids, and the anterior conjunctival vessels belonging to the system of the anterior ciliary arteries. The posterior conjunctival vessels feed the conjunctiva of the cartilage, transitional fold and eyeball, with the exception of the peri-limbus.
Noah zone, which is supplied by the anterior conjunctival vessels. The anterior and posterior conjunctival arteries are connected by anastomoses.
Conjunctival veins accompany arteries, but their branches are more numerous. Some of them flow into the veins of the face, and others into the orbital vein system. Lymph, vessels of the conjunctiva of the eyelids form a dense network lying in the subconjunctival tissue. The direction of these vessels coincides with the course of the blood vessels - from the temporal half of the lymphatic conjunctiva, the vessels go to the preauricular node, and from the nasal one to the submandibular lymph nodes.
Sensory nerves The conjunctiva receives from the first branch of the trigeminal nerve - the optic nerve (n. Ophthalmicus). Its branch - the lacrimal nerve (n. Lacrimalis) - innervates the temporal part of the conjunctiva of the upper and partly the lower eyelid; the supraorbital nerve (n. supraorbitalis) and the supra-block nerve (n. supratrochlearis) supply the nasal conjunctiva of the upper eyelid. From the second branch of the trigeminal nerve - the maxillary nerve (n. Maxillaris), the zygomatic nerve (n. Zygomaticus), which supplies the temporal half of the conjunctiva of the lower eyelid, and the infraorbital nerve (n. Infraorbitalis), which supplies its nasal half, branch off.
Physiology
The abundance of sensitive innervation in the Conjunctiva provides a protective function - when the smallest foreign bodies enter, the secretion of lacrimal fluid increases, blinking movements become more frequent, as a result of which the foreign body is mechanically removed from the conjunctival sac. The secret of the conjunctival glands, constantly wetting the surface of the eyeball, acts as a lubricant that reduces friction during its movements, protects the cornea from drying out and preserves its transparency. The barrier function of the Conjunctiva is carried out due to the content of enzymes (lysozyme and others) in the lacrimal fluid and the abundance of lymphoid elements in the submucous adenoid tissue.
Pathology
Symptomatology. Color change. Hyperemia of the Conjunctiva is noted with its inflammation (see the complete body of knowledge Conjunctivitis), with non-inflammatory stagnation of blood; blanching of the conjunctiva - with general anemia. Pigmentation of the conjunctiva of the sclera is observed in various general diseases of the body: yellow color - with jaundice, yellow-brown - with Addison's disease, slate-gray - with argyrosis (see the complete body of knowledge).
In the conjunctiva, hemorrhages are also observed - with trauma, inflammation, with an increase in blood pressure, and so on.
Edema of the conjunctiva (chemosis) occurs very often under various conditions: in addition to inflammation of the conjunctiva or adjacent tissues, it is observed with stagnation of blood and lymph in the orbital region, for example, with eye socket tumors, with exophthalmos (see the complete body of knowledge), as well as with anemia, nephritis, etc. With severe edema, the Conjunctiva moves to the edges of the cornea in the form of a vitreous shaft.
Emphysema of the conjunctiva occurs simultaneously with emphysema of the eyelids (see the complete body of knowledge) with damage to the walls of the orbit, as a result of which conditions are created for the entry of air under the conjunctiva from the surrounding paranasal sinuses.
Diseases. Lymphangiectasia of the conjunctiva is a common phenomenon, especially in the area of the conjunctiva of the sclera; characterized by the appearance under the epithelium of the Conjunctiva of roundish watery vesicles the size of a pinhead, which are often multiple and, merging with each other, sometimes form small translucent lymphatic cysts. Treatment consists of puncturing or removing them.
Conjunctival tuberculosis is a rare disease; usually occurs endogenously as a secondary process or as a result of spread from affected tissues. The tuberculous process often affects the conjunctiva of the upper eyelid; It usually manifests itself as an ulcer with pitted edges and a cheesy or greasy bottom. At the bottom of the ulcer and in the surrounding Conjunctiva, grayish nodules are visible. Sometimes tuberculosis of the Conjunctiva manifests itself in the form of papillomatous growths (see color picture 7), in which you can see its characteristic nodules. The course of tuberculosis of the Conjunctiva is chronic with a tendency to relapse. General and local treatment (streptomycin, PASK, ftivazid and others).
Pemphigus of the eye (pemphigus) is a rare disease, the characteristic symptom of which is the formation of blisters on the conjunctiva, as well as on the cornea and skin of the eyelids. The etiology of ocular pemphigus is unknown; it is believed to be of viral origin. It can occur with a general severe, chronic disease of the body with a gradual lesion of all areas of the skin and mucous membranes by the pemphigus process. On the conjunctiva of the eyelids and transitional folds, bubbles of various sizes are formed, they quickly burst, and flat erosions, covered with fibrinous plaque, remain in their place; limited ulceration is less common. Many ophthalmologists also refer to the ophthalmic pemphigus as essential cicatricial wrinkling of the Conjunctiva, in which from the very beginning of the disease there are scars on the conjunctiva with abnormal growth of individual eyelashes, and the increase in the process leads to wrinkling of the conjunctiva, symblepharon. The prognosis is poor: treatment is unsuccessful, the disease always ends in blindness in both eyes.
Dystrophic processes. These include amyloidosis, pinguecula, pterygoid hymen (see complete body of knowledge Pterygium), xerosis, or dryness, Conjunctiva (see complete body of knowledge Xerophthalmia), simblefaron, epitarsus.
Amyloidosis of the conjunctiva is a kind of lesion of unclear etiology. It can be a manifestation of general amyloidosis (see the complete body of knowledge) or a local disease, which is often preceded by any chronic inflammatory disease of the Conjunctiva, for example, trachoma, or an independent disease of the Conjunctiva. It begins gradually, without inflammation, usually from transitional folds, spreading to the conjunctiva of the cartilage, the lunate fold, sometimes capturing the cartilage tissue. Initially, there is a thickening of the Conjunctiva, then tuberous growths appear in it, waxy, sometimes translucent and slightly gelatinous. In the future, the thickening of the Conjunctiva increases, protrudes into the region of the palpebral fissure and the patient can hardly open the eyelids. Pathoanatomically, there is a thickening or thinning of the epithelium of the Conjunctiva, and under it is an accumulation of homogeneous masses that react to amyloid or hyaline, the presence of infiltration from plasma cells. Treatment - surgical removal of a part of the reborn conjunctiva
Pinguecula (wen) is a small yellowish-white formation, slightly elevated, round or triangular in shape, often developing in the elderly under the influence of a variety of prolonged external stimuli. Pathoanatomically, in addition to keratinization of the epithelium, the main change is dystrophy (hyaline degeneration) of the subepithelial tissue. The pinguecula is promptly removed only for cosmetic reasons.
Simblefaron - cicatricial fusion of the conjunctiva of the eyelid with the conjunctiva of the eyeball. Simblefaron occurs after burns, eye diphtheria, pemphigus, wounds, and so on, when wound or ulcerative surfaces form on the opposite surfaces of the conjunctiva of the eyelid and eyeball, which subsequently grow together. Distinguish between anterior and posterior simblefaron: if the conjunctival vault is not destroyed - the simblefaron is anterior; if the fornix does not exist, the posterior symblepharon. A species of special origin is the posterior symblepharon, which is formed as a result of widespread scarring of the conjunctiva during trachoma with smoothing of the transitional folds and a decrease in the entire conjunctival sac. Surgical treatment: plastic surgery on the conjunctiva
Epitarsus is a duplicate of the mucous membrane of the eyelid between the fornix of the Conjunctiva and the cartilage of the upper eyelid; looks like a lining of a whitish color with a smooth surface penetrated by blood vessels. The appearance of epitarsus is due to incomplete closure of the frontal-maxillary cleft (congenital anomaly). Not subject to treatment.
Tumors. Benign. Fibroids of the Conjunctiva, consisting of papillary growths of connective tissue, have a smooth surface, soft or dense consistency, capable of rapid growth, especially in the area of the lacrimal caruncle. Soft fibroids bleed frequently. Conjunctiva papillomas are close to them in structure, which, in contrast to fibroids, have an uneven surface, similar to a mulberry or cauliflower. They are more often localized on the conjunctiva of the eyeball, mainly at the limbus, from where they can spread to the cornea. Papillomas often recur and, with malignancy, are subject to surgical treatment.
Hemangiomas and lymphangiomas occur both initially in the conjunctiva and spreading to it from the eyelids. Hemangiomas (see the complete body of knowledge) are more often located on the conjunctiva of the eyeball, have a mesodermal nature and are congenital in nature. Removal of hemangiomas is dictated in some cases by cosmetic considerations, in others by dysfunction of the eye caused by them or by the occurrence of bleeding. Surgical removal of hemangioma with preliminary ligation, vascular chipping or cauterization with diathermocoagulation is performed. Close-focus X-ray therapy is also used. Lymphangiomas (see full body of knowledge) are very rare.
Dermoid and lipodermoid are congenital tumors. Dermoids of the Conjunctiva are clinically small, rounded formations with clear boundaries, whitish or yellowish in color (color table, Art. 289, Figure 5); they are usually located on the lower outer edge of the cornea and somewhat capture its periphery, motionless, of dense consistency. The surface of the dermoids is similar to the skin: the superficial layers of the epithelium are keratinized, underneath there is a dense fibrous connective tissue and in it hair follicles, sebaceous and sometimes sweat glands. Simultaneously with dermoids, other anomalies of the development of the eye (colobomas of the eyelids, irises, and others) can occur. The lipodermoid is characterized by the location under the Conjunctiva in the equatorial region of the eye between the superior rectus and the external rectus muscles in the form of a thick fold of the Conjunctiva, which comes out from under the eyelid with its edge and is lost posteriorly in the depth of the orbit. Lipodermoid contains in its thickness more adipose tissue than dermoid, and therefore has a more yellowish color and softer consistency; he is more mobile. Treatment of both formations is surgical removal.
Nevus Conjunctiva - pigmented and non-pigmented birthmarks (see the complete body of knowledge Nevus). Non-pigmented spots Conjunctiva in the form of flat yellowish elevations with a smooth surface are most often located near the limbus of the cornea. They can become malignant. In the absence of growth, the nevus cannot be treated.
Malignant. Epithelioma, or carcinoma, is more often localized in the limbus, where the conjunctiva is most often exposed to external stimuli. Pathological anatomical epitheliomas of the Conjunctiva in most cases are squamous cell carcinoma (see the complete body of knowledge) with a tuberous surface prone to superficial ulceration and papillomatous growths of a whitish-gray or pinkish-yellow color, depending on the number of vessels. Elements of the epithelioma, growing into the tissue of the cornea and the conjunctiva, tend to penetrate into the orbit, surround the surface of the eyeball, forming peribulbar epitheliomas. In the initial stages, X-ray therapy is possible; surgical intervention is also indicated - thorough removal of the tumor, and when germinating into the orbit - exenteration of the orbit (see the complete body of knowledge).
Melanoma of the Conjunctiva is not uncommon. It develops from a preexisting pigmented birthmark in the limbus, lacrimal carcinoma or lunate fold, and has the appearance of smooth or bumpy tumors of a dark color (see color picture 6). Melanoma (see full body of knowledge) often gives relapses and metastases, especially after unsuccessful surgery. In the earliest stages, in the absence of active growth of melanoma, one should refrain from surgery. When the tumor grows or in case of relapse, it may be necessary to remove the eye or even exenterate the orbit.
Are you totally unhappy with the prospect of irrevocably disappearing from this world? You do not want to end your life path in the form of a disgusting rotting organic mass devoured by the grave worms swarming in it? Do you want to return to your youth to live one more life? Start all over again? Fix the mistakes you made? Make unfulfilled dreams come true? Follow this link:
but) Anatomy of the conjunctiva of the eye... The conjunctiva is a thin, transparent, vascularized mucous membrane that lines the inner surface of the eyelids and the anterior surface of the eyeball to the limbus. This tissue forms a kind of a bag and consists of the palpebral part (covering the inner surface of the eyelids), the bulbar part (covering the surface of the sclera), the conjunctiva of the arches and the medial semilunar fold.
The palpebral conjunctiva is supplied by the same vessels as the eyelids, while the bulbar conjunctiva receives its blood supply from the anterior ciliary arteries. The innervation of the conjunctiva is carried out by the lacrimal, supraorbital, supra-block and infraorbital branches of the orbital branch of the trigeminal nerve.
The thickness of the conjunctival epithelium varies and ranges from two to five cells, at the level of the limbus it continues into the epithelium of the cornea, and at the edge of the eyelid - into the skin. The bulbar conjunctiva is lined with non-keratinizing stratified squamous epithelium, the fornix conjunctiva and tarsal conjunctiva are covered, respectively, with cylindrical and cubic epithelium.
The main feature of the cellular structure of the conjunctiva is the presence of goblet cells, which make up 10% of the basal cells of the conjunctival epithelium. These cells predominate in the medial part of the fornix and palpebral zone and play an essential role in the secretion of the mucin component of the tear film. The number of these cells increases with chronic inflammation of the conjunctiva, and decreases with pemphigoid and vitamin A deficiency. Other cells lying between the layers of the epithelium are melanocytes, Langerhans cells and intraepithelial lymphocytes.
Under the epithelium lies loose tissue, its own substance - the substantia propria. It contains various cells involved in the immune response (mast cells, plasma cells, eosinophils and lymphocytes) scattered throughout the vasculature. This vascular clump of immune cells, commonly referred to as conjunctival-associated lymphoid tissue, is constantly exposed to infection and allergens from the environment, creating ideal conditions for inflammation to develop.
Under the conjunctiva lies a layer of fibroelastic tissue, the Tenon's capsule, which surrounds the eyeball from the corneoscleral junction to the optic nerve. In children, the Tenon capsule is thicker and contains more fibroblasts. Therefore, surgeries such as trabeculectomy in children, especially without adjuvant treatment, such as intraoperative antimetabolites, may be ineffective due to the aggressive healing response induced by these fibroblasts.
b) Conjunctiva in systemic diseases... A thorough examination of the conjunctiva with a flashlight in bright light conditions can often provide comprehensive information about the existing systemic disease. Changes in color, gloss, abnormalities in vascularization and pigmentation allow assumptions about local or systemic causes that caused them. Then, a slit lamp examination is performed in order to examine in detail the zone of pathological changes.
1. Conjunctiva with vitamin A deficiency... This is a systemic pathology that causes changes in various organs. Ocular manifestations are called xerophthalmia, patients have hemeralopia, conjunctival and corneal xerosis, Bitot plaques, keratomalacia and "xerophthalmic" fundus.
In this state, the epithelium of the conjunctiva is transformed from a normal cylindrical to a multilayered flat one. This is accompanied by the disappearance of goblet cells, the formation of a layer of granular cells and keratinization of the surface. The conjunctiva loses its normal luster and becomes dry and non-wetting. The defeat is almost always bilateral. The classic ophthalmic symptom is Bitot spots, which are superficial scaly gray areas in the interpalpebral region of the bulbar conjunctiva. These spots can be colonized by Corynebacterium xerosis, due to their gas-generating properties, Bitot spots appear to be foamy.
If untreated, the process spreads to the cornea and causes corneal xerosis, which ultimately leads to its melting - keratomalacia.
The diagnosis of xerophthalmia is often made clinically and does not require any additional research. In doubtful cases, an impression cytological study of the superficial layers of the conjunctival epithelium reveals the disappearance of goblet cells and keratinization of the epithelium. Oral vitamin A is preferred because it is safe, cost effective, and effective.
Sick children over 12 months of age should be given retinol palmitate (110 mg) or retinol acetate (200,000 IU) orally as the initial dose, which is repeated the next day. An additional dose is given two weeks later to increase liver stores. Children 6 to 11 months of age should be given half of the indicated dose, and children under six months of age should be given a quarter of that dose.
Parenteral administration is indicated for children with conditions such as persistent vomiting, severe stomatitis with concomitant swallowing disorders, severe diarrhea with malabsorption, and septic shock. These children are treated with an intramuscular injection of 55 mg of water-soluble retinol palmitate (100,000 IU) instead of the first oral dose. Doing is repeated the next day. Children under the age of one year are prescribed vitamin A at half the dosage. After the end of the acute phase, dietary support is necessary with food rich in provitamin A.
Spot Bitot.Superficial scaly foamy Bitot spot of the bulbar conjunctiva.
 Xerophthalmia... Bulbar conjunctiva in the lower regions dry, matte, wrinkled.
Xerophthalmia... Bulbar conjunctiva in the lower regions dry, matte, wrinkled. Concomitant corneal xerosis is visible.
2. Conjunctiva with xeroderma pigmentosa (Xeroderma pigmentosa). This condition is inherited in an autosomal recessive manner. Symptoms manifest in early childhood. Patients develop severe photophobia, photosensitivity, and typical dark skin pigmentation. There is an increased risk of developing malignant neoplasms exposed to solar irradiation of mucocutaneous structures and eyes. The ability to restore DNA molecules damaged by ultraviolet radiation is impaired, which leads to the accumulation of damaged DNA, causing chromosomal mutations and cell death, which explains the development of neoplasms in such patients.
The conjunctiva of the interpalpebral zone is mainly affected, xerosis, telangiectasia, constant discharge from the conjunctival cavity, pigmentation, pinguecula and pterygium develop. Neoplasms of the surface of the eye, such as squamous cell carcinoma, basal cell carcinoma, and malignant melanoma, may develop and mainly affect the limbus. Corneal changes include xerotic keratitis, ribbon-like nodular keratopathy, scarring, ulceration, vascularization, and perforation. The posterior segment is usually unchanged. Symptomatic conjunctival nodules protruding above the surface and suspicious neoplasms may require repeated excision; in other cases, treatment is symptomatic.
3. Conjunctiva in Sturge-Weber syndrome... This congenital disease is characterized by the classic triad: cutaneous facies angioma, pia mater angioma and eye lesions. Facial angioma usually develops in the area of innervation of the orbital branch of the trigeminal nerve. Usually there is an expansion of episcleral and conjunctival vessels with the formation of aneurysms in the limbus. These changes are often accompanied by glaucoma, especially in patients with severe conjunctival involvement.
4. Conjunctiva with ichthyosis... Ichthyosis is a heterogeneous family of at least 28 genetic skin diseases. In most cases, there is an autosomal dominant or X-linked inheritance mechanism. There is a rare autosomal recessive form - lamellar ichthyosis. In all these conditions, dry scaly elements develop mainly on the skin of the upper half of the body, mainly around the neck, mouth and trunk. Primary or secondary inflammation of the conjunctiva may develop due to eyelid abnormalities such as ectropion. A papillary reaction may also occur. Treatment consists of prescribing appropriate lubricants and correcting eyelid abnormalities, if any.
5. Conjunctiva at... Conjunctival pallor is a sensitive and commonly used symptom of anemia in children. This symptom is best assessed in bright sunlight and in conjunction with other systemic changes. An important etiological factor, especially in developing countries, is systemic helminthiasis. Pallor of the conjunctiva can be masked by conjunctival inflammation, especially trachoma.
6. Conjunctiva with leukemia... The defeat of the conjunctiva with leukemia is rare. It occurs in about 4% of patients. However, damage to the conjunctiva may be the first sign of illness or recurrence. Therefore, early diagnosis is of great importance. Initially, the lesion is manifested by injection of the bulbar (especially the perilimbal zone) or palpebral conjunctiva. Sometimes the conjunctiva is erythematous and chemotic. The lesion is dense, painless, and often accompanied by subconjunctival hemorrhage. Cellular infiltration of all layers of its own substance is histologically revealed. Infiltration can be diffuse or fragmented and is usually seen around blood vessels. Conjunctival lesions usually quickly regress with systemic chemotherapy.
7. Measles keratoconjunctivitis... Keratoconjunctivig in measles is usually bilateral. Typical Koplik-Filatov spots can be found on the conjunctiva. Edema of the lunate fold may develop. After that, in children in the early stages, in adults, epithelial keratitis may develop later. In patients in the absence of impaired immunity and normal nutrition, these changes usually disappear without a trace. Treatment is symptomatic; local anti-inflammatory drugs can alleviate the course of the disease. But in children with protein-energy malnutrition, this disease can be especially difficult. It can also occur in children with vitamin A deficiency, in such cases keratomalacia can develop rapidly. In immunocompromised patients, a secondary bacterial infection often occurs.
8. Conjunctiva with alkaptonuria... It is a rare autosomal recessive disorder in which a person's urine turns dark brown to black when exposed to air. It is associated with the pathology of chromosome 3q21-q24 and is caused by a deficiency of homogentisine 1,2-dioxygenase, leading to the accumulation of homogentisic acid in various tissues and organs. Systemic changes include facial and nail pigmentation, calcifying and atherosclerotic heart disease, and arthritis. Ocular manifestations include brown or black pigmentation of the nasal or temporal sclera at the insertion of the horizontal rectus muscles. Corneal pigmentation has been described.
9. Conjunctiva in ataxia telangiectasia (Louis Bar syndrome). This rare autosomal recessive disorder is characterized by early-onset cerebellar ataxia, oculomotor telangiectasia, oculomotor apraxia, dysarthria, and immunodeficiency. Of all these disorders, ataxia develops first and progresses. Fragility of chromosomes and increased sensitivity to ionizing radiation determines the predisposition to the development of malignant diseases, including lymphomas and leukemias. In patients, as a rule, high levels of alpha-fetoproteins in the blood are determined.
The most common ocular changes are conjunctival telangiectasia, usually in the first decade of life. Typically, telangiectasias appear on the interpalpebral bulbar conjunctiva, but may extend into the fornices. Caused by exposure to ultraviolet radiation, these changes can be prevented or minimized by early, consistent use of glasses with 100% UV blocking lenses. Other comorbid disorders include hypometric saccades, horizontal oculomotor apraxia, lack of accommodation, strabismus, and nystagmus.
10. Conjunctiva in Fabry disease... This X-linked disease is a lysosomal storage disease caused by a deficiency of alpha-galactosidase A, which degrades the glycosphingolipid components of plasma membranes. Deficiency of this enzyme leads to the accumulation of glycosphingolipids, especially globotriaosilceramide. Common manifestations are tortuosity of the conjunctival vessels, telangiectasia, and vortex keratopathy (cornea verticellata).
11. Conjunctiva in Randu-Weber-Osler syndrome... It is a rare autosomal dominant blood vessel disorder that can cause severe bleeding. It is characterized by vasodilatation of various organs and systems. Systemic manifestations include epistaxis, dyspnea on exertion, gastrointestinal bleeding, hemoptysis, and hematuria. Conjunctival telangiectasia is a classic detectable ocular anomaly. It can manifest as bloody tears or obvious external bleeding. Telangiectasias and retinal arteriovenous malformations have been described. These vessels are stable and differ from newly formed vessels by the absence of leakage during fundus fluorescence angiography.
12. Conjunctiva in sickle cell anemia... Changes in the conjunctiva in this disease are extremely specific. In the inferior temporal quadrant of the pallid conjunctiva, microaneurysms of capillaries and venules in the form of a comma are revealed, which disappear under the influence of the heat of the illuminator. These aneurysms reappear after instillation of a weak vasoconstrictor drug. Vascular abnormalities worsen during sickle cell crises.
2-12-2012, 16:49
Description
The structure and function of the conjunctiva
The connective membrane of the eye, or conjunctiva, is the mucous membrane that lines the eyelids from the back and extends to the eyeball all the way to the cornea and thus connects the eyelid to the eyeball. When the palpebral fissure is closed, the connecting sheath forms a closed cavity - conjunctival sac, which is a narrow slit-like space between the eyelids and the eyeball.
The mucous membrane that covers the back of the eyelids is called conjunctival eyelid, and the covering sclera - conjunctiva of the eyeball or sclera... The part of the conjunctiva of the eyelids, which, forming the vaults, passes to the sclera, is called the conjunctiva of the transitional folds or the vault. Accordingly, the upper and lower conjunctival vaults are distinguished. At the inner corner of the eye, in the region of the third eyelid rudiment, the conjunctiva forms a vertical semilunar fold and a lacrimal meatus.
In the conjunctiva, two layers are distinguished - epithelial and subepithelial... The conjunctiva of the eyelids is tightly fused with the cartilaginous plate. The epithelium of the conjunctiva is multilayered, cylindrical with a large number of goblet cells. The conjunctiva of the eyelids is smooth, shiny, pale pink, yellowish columns of meibomian glands passing through the thickness of the cartilage are visible through it. Even with the normal state of the mucous membrane at the outer and inner corners of the eyelids, the conjunctiva covering them looks slightly hyperemic and velvety due to the presence of small papillae.
The conjunctiva of the transitional folds is loosely connected to the underlying tissue and forms folds that allow the eyeball to move freely. The fornix conjunctiva is covered with stratified squamous epithelium with a small number of goblet cells. Subepithelial layer represented by loose connective tissue with inclusions of adenoid elements and accumulations of lymphoid cells in the form of follicles. The conjunctiva contains a large number of Krause lacrimal glands.
The conjunctiva of the sclera is tender, loosely connected to the episcleral tissue. The stratified squamous epithelium of the conjunctiva of the sclera smoothly passes onto the cornea.
The conjunctiva borders on the skin of the edges of the eyelids, and on the other hand, on the corneal epithelium. Diseases of the skin and cornea can spread to the conjunctiva, while diseases of the conjunctiva can spread to the skin of the eyelids (blepharoconjunctivitis) and the cornea (keratoconjunctivitis). Through the lacrimal opening and the lacrimal canal, the conjunctiva is also connected with the mucous membrane of the lacrimal sac and nose.
Conjunctiva profuse supplied with blood from the arterial branches of the eyelids, as well as from the anterior ciliary vessels. Any inflammation and irritation of the mucous membrane is accompanied by a bright hyperemia of the vessels of the conjunctiva of the eyelids and vaults, the intensity of which decreases towards the limbus.
Due to the dense network of nerve endings of the first and second branches of the trigeminal nerve, the conjunctiva plays the role of integumentary sensitive epithelium.
Basic physiological function of the conjunctiva- eye protection: if a foreign body gets in, irritation of the eye appears, the secretion of lacrimal fluid increases, blinking movements become more frequent, as a result of which the foreign body is mechanically removed from the conjunctival cavity. The secret of the conjunctival sac constantly wets the surface of the eyeball, reduces friction during its movements, and helps to preserve the transparency of the moist cornea. This secret is rich in protective elements: immunoglobulins, lysozyme, lactoferrin. The protective role of the conjunctiva is also provided due to the abundance of lymphocytes, plasma cells, neutrophils, mast cells and the presence of immunoglobulins of all five classes.
Diseases of the conjunctiva
Among the diseases of the conjunctiva, the main place is occupied by inflammatory diseases. Conjunctivitis- this is an inflammatory reaction of the conjunctiva to various influences, characterized by hyperemia and edema of the mucous membrane; swelling and itching of the eyelids, separated from the conjunctiva, the formation of follicles or papillae on it; sometimes accompanied by damage to the cornea with visual impairment.
Conjunctival hyperemia- an alarming signal common to many eye diseases (acute iritis, an attack of glaucoma, ulcer or corneal trauma, scleritis, episcleritis), therefore, when establishing a diagnosis of conjunctivitis, it is necessary to exclude other diseases accompanied by eye redness.
The following three groups of conjunctival diseases have fundamental differences:
- infectious conjunctivitis (bacterial, viral, chlamydial);
- allergic conjunctivitis (hay fever, spring catarrh, drug allergy, chronic allergic conjunctivitis, large papillary conjunctivitis);
- dystrophic diseases of the conjunctiva (keratoconjunctivitis dry, pinguecula, pterygium).
Infectious conjunctivitis
Bacterial conjunctivitis
Any of the widespread pathogens of a purulent infection can cause inflammation of the conjunctiva. Cocci, especially staphylococci, are the most common cause of conjunctival infection, but it proceeds more favorably. The most dangerous pathogens are Pseudomonas aeruginosa and gonococcus causing severe acute conjunctivitis, in which the cornea is often affected (Figure 9.1).
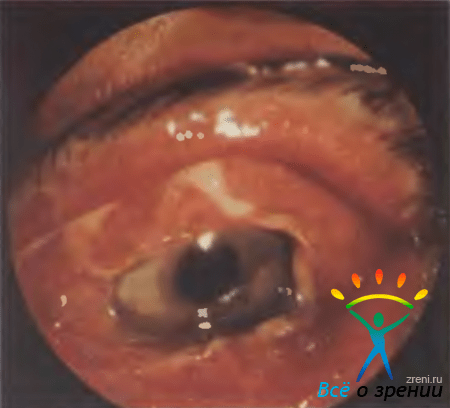
Rice. 9.1. Acute bacterial conjunctivitis.
Acute and chronic conjunctivitis caused by staphylococcus ... Acute conjunctivitis occurs more often in children, less often in the elderly, and even less often in middle-aged people. Usually, the pathogen enters the eye from the hands. First, one eye is affected, after 2-3 days the other. The clinical manifestations of acute conjunctivitis are as follows. In the morning, the patient can hardly open his eyes, as the eyelids stick together. When the conjunctiva is irritated, the amount of mucus increases. The nature of the discharge can rapidly change from mucous to mucopurulent and purulent. The discharge drains over the edge of the eyelid, dries up on the eyelashes. External examination reveals hyperemia of the conjunctiva of the eyelids, transitional folds and sclera. The mucous membrane swells, loses its transparency, the pattern of the meibomian glands is erased. The severity of superficial conjunctival vascular infection decreases towards the cornea. The patient is worried about discharge on the eyelids, itching, burning sensation and photophobia.
Chronic conjunctivitis develops slowly, proceeds with periods of improvement. Patients are worried photophobia, slight irritation and rapid eye fatigue. The conjunctiva is moderately hyperemic, loosened, dry discharge (crusts) along the edge of the eyelids. Conjunctivitis can be associated with nasopharyngeal disease, otitis media, sinusitis. In adults, conjunctivitis often occurs with chronic blepharitis, dry eye syndrome, damage to the lacrimal duct.
To identify a bacterial infection in conjunctivitis of newborns and acute conjunctivitis, microscopic examination of smears and cultures of discharge from the conjunctiva is used. The isolated microflora is examined for pathogenicity and sensitivity to antibiotics.
In treatment, the main place is occupied by local antibiotic therapy: instill sodium sulfacyl, vitabact, futsitalmic, 3-4 times a day, or lay an eye ointment: tetracycline, erythromycin, "..." a, 2-3 times a day. In acute course, eye drops are prescribed tobrex, ocacin, "..." up to 4-6 times a day. With edema and severe irritation of the conjunctiva, instillations of antiallergic or anti-inflammatory drops (alomid, lecrolin or naklof) are added 2 times a day.
In acute conjunctivitis, it is impossible to tie and glue the eye, since under the bandage favorable conditions are created for the multiplication of bacteria, the threat of corneal inflammation increases.
Acute conjunctivitis caused by Pseudomonas aeruginosa ... The disease begins acutely: there is a large or moderate amount of purulent discharge and edema of the eyelids, the conjunctiva of the eyelids is sharply hyperemic, bright red, edematous, loosened. Without treatment, conjunctival infection can easily spread to the cornea and cause a rapidly progressive ulcer to form.
Treatment: instillation of antibacterial eye drops (tobrex, ocacin, "..." or gentamicin) in the first 2 days 6-8 times a day, then up to 3-4. The most effective combination of two antibiotics, for example, tobrex + ocacin or gentamicin + polymyxin. When the infection spreads to the cornea, tobramycin, gentamicin or ceftazidime are injected parabulbar and tavanic in tablets or gentamicin, tobramycin in the form of injections are systemically used. With pronounced edema of the eyelids and conjunctiva, antiallergic and anti-inflammatory drops (spersallerg, allergophthal or naklof) are additionally installed 2 times a day. In case of damage to the cornea, metabolic therapy means are needed - drops (taufon, vitasik, carnosine) or gels (corneregel, solcoseryl).
Acute conjunctivitis caused by gonococcus ... Venereal disease. sexually transmitted infection (direct genital-eye contact or genital-hand-eye transmission). Hyperactive purulent conjunctivitis is characterized by rapid progression. The eyelids are edematous, the discharge is profuse, purulent, the conjunctiva is sharply hyperemic, bright red, irritated, gathers in protruding folds, often there is edema of the scleral conjunctiva (chemosis). Keratitis develops in 15-40% of cases, at first superficial, then a corneal ulcer forms, which can lead to perforation after 1 to 2 days.
In acute conjunctivitis, presumably caused by Pseudomonas aeruginosa or gonococcus, treatment is started immediately, without waiting for laboratory confirmation, since a delay of 1-2 days can lead to the development of corneal ulcers and eye death.
Treatment: in case of gonococcal conjunctivitis, confirmed by laboratory or suspected on the basis of clinical manifestations and anamnesis of the disease, antibacterial therapy is first performed: rinsing the eye with a solution of boric acid, instillation of eye drops (ocacin, "..." or penicillin) 6-8 times a day. Systemic treatment is carried out: quinolone antibiotic 1 tablet 2 times a day or intramuscular penicillin. Additionally, instillations of anti-allergic or anti-inflammatory drugs (spersallerg, allergophthal or naklof) are prescribed 2 times a day. In case of keratitis symptoms, vitasik, carnosine or taufon are also instilled 2 times a day.
A particular danger is gonococcal conjunctivitis in newborns (gonoblennorrhea)... Infection occurs during the passage of the fetus through the birth canal of a mother with gonorrhea. Conjunctivitis usually develops 2-5 days after birth. Swollen, dense, bluish-purple eyelids are almost impossible to open for examination of the eye. When pressed, bloody-purulent discharge is poured out of the palpebral fissure. The conjunctiva is sharply hyperemic, loosened, bleeds easily. The exclusive danger of gonoblenorrhea is damage to the cornea up to the death of the eye. Local treatment is the same as in adults, and systemic - the introduction of antibacterial drugs in doses corresponding to age.
Diphtheria conjunctivitis ... Diphtheria of the conjunctiva, caused by a diphtheria bacillus, is characterized by the appearance on the conjunctiva of the eyelids with grayish films that are difficult to remove. The eyelids are dense, edematous. A cloudy liquid with flakes is released from the palpebral fissure. The films are tightly welded to the underlying tissue. Their separation is accompanied by bleeding, and after necrotization of the affected areas, scars are formed. The patient is isolated in the infectious diseases department and treated according to the diphtheria therapy regimen.
Viral conjunctivitis
Viral conjunctivitis is common and occurs in the form of epidemic outbreaks and episodic diseases.
Epidemic keratoconjunctivitis ... Adenoviruses (more than 50 of their serotypes are already known) cause two clinical forms of eye damage: epidemic keratoconjunctivitis, which is more severe and accompanied by damage to the cornea, and adenoviral conjunctivitis, or pharyngoconjunctival fever.
Epidemic keratoconjunctivitis is hospital infection, more than 70% of patients become infected in medical institutions. The source of infection is a patient with keratoconjunctivitis. The infection spreads by contact, less often by airborne droplets. Factors of transmission of the pathogen are infected hands of medical personnel, reusable eye drops, tools, devices, eye prostheses, contact lenses.
The duration of the incubation period of the disease is 3-14, more often 4-7 days. The duration of the infectious period is 14 days.
The onset of the disease is acute, usually both eyes are affected: first one, after 1-5 days the second. Patients complain of pain, sensation of a foreign body in the eye, lacrimation. The eyelids are edematous, the conjunctiva of the eyelids is moderately or significantly hyperemic, the lower transitional fold is infiltrated, folded, in most cases small follicles and punctate hemorrhages are revealed.
After 5-9 days from the onset of the disease, stage II of the disease develops, accompanied by the appearance of characteristic point infiltrates under the corneal epithelium. With the formation of a large number of infiltrates in the central zone of the cornea, vision decreases.
Regional adenopathy - an increase and soreness of the parotid lymph nodes - appears on the 1-2 day of the disease in almost all patients. The defeat of the respiratory tract is observed in 5-25% of patients. The duration of epidemic keratoconjunctivitis is up to 3-4 weeks. As studies carried out in recent years have shown, a serious consequence of adenovirus infection is the development of dry eye syndrome due to impaired production of lacrimal fluid.
Laboratory diagnostics of acute viral conjunctivitis (adenoviral, herpesvirus) includes a method for determining fluorescent antibodies in conjunctival scrapings, polymerase chain reaction and, less often, a method for isolating the virus.
Treatment is fraught with difficulties, since there are no drugs selectively affecting adenoviruses. They use drugs of broad antiviral action: interferons (lokferon, ophthalmoferon, etc.) or interferon inducers, instillations are carried out 6-8 times a day, and on the 2nd week, reducing their number to 3-4 times a day. In the acute period, the antiallergic drug allergophthal or spersallerg is additionally instilled 2-3 times a day and antihistamines are taken orally for 5-10 days. In cases of subacute course apply drops of alomid or lecrolin 2 times a day. With a tendency to film formation and during the period of corneal eruptions, corticosteroids (dexapos, maxidex or ophtan-dexamethasone) are prescribed 2 times a day. For corneal lesions, taufon, carnosine, vitasik or korneregel are used 2 times a day. In cases of a lack of tear fluid for a long period of time, tear substitutes are used: natural tear 3-4 times a day, Oftagel or Vidisik-gel 2 times a day.
Prevention of nosocomial adenovirus infection includes the necessary anti-epidemic measures and measures of the sanitary and hygienic regime:
- examination of the eyes of each patient on the day of hospitalization to prevent the introduction of infection into the hospital;
- early detection of cases of development of diseases in a hospital;
- isolation of patients in isolated cases of disease and quarantine in outbreaks, anti-epidemic measures;
- sanitary and educational work.
Adenoviral conjunctivitis ... The disease is milder than epidemic keratoconjunctivitis, and rarely causes outbreaks of nosocomial infection. The disease usually occurs in children's groups. The pathogen is transmitted by airborne droplets, less often by contact. The incubation period lasts 3-10 days.
The symptoms of the disease are similar to the initial clinical manifestations of epidemic keratoconjunctivitis, but their intensity is much lower: the discharge is scanty, the conjunctiva is hyperemic and moderately infiltrated, there are few follicles, they are small, sometimes there are punctate hemorrhages. In 1/2 of the patients, regional adenopathy of the parotid lymph nodes is found. Point epithelial infiltrates may appear on the cornea, but they disappear without a trace, without affecting visual acuity.
For adenoviral conjunctivitis common symptomatology: damage to the respiratory tract with fever and headache. Systemic damage may precede eye disease. The duration of adenoviral conjunctivitis is 2 weeks.
Treatment includes instillation of interferons and antiallergic eye drops, and in case of insufficient lacrimal fluid - artificial tears or ophtagel.
Prophylaxis nosocomial spread of infection is the same as in epidemic keratoconjunctivitis.
Epidemic hemorrhagic conjunctivitis (EHC) ... EGC, or acute hemorrhagic conjunctivitis, has been described relatively recently. The first EGC pandemic began in 1969 in West Africa and then spread to North Africa, the Middle East and Asia. The first outbreak of EGC in Moscow was observed in 1971. Epidemic outbreaks in the world occurred in 1981-1984 and 1991-1992. The disease requires close attention, since EGC outbreaks in the world are repeated with a certain frequency.
The causative agent of EGC is enterovirus-70... EGC is characterized by a short incubation period, which is unusual for a viral disease - 12-48 hours. The main route of infection spread is contact. There is a high contagiousness of EGC, the epidemic is "explosive". In eye hospitals, in the absence of anti-epidemic measures, 80-90% of patients can be affected.
Clinical and epidemiological features of EGC so characteristic that on their basis the disease can be easily distinguished from other ophthalmic infections. The onset is acute, first one eye is affected, after 8-24 hours - the second. Due to severe pain and photophobia, the patient seeks help on the first day. The mucous or mucopurulent discharge from the conjunctiva, the conjunctiva is sharply hyperemic, subconjunctival hemorrhages are especially characteristic: from point petechiae to extensive hemorrhages, involving almost the entire conjunctiva of the sclera (Fig. 9.2).

Rice. 9.2. Epidemic hemorrhagic conjunctivitis.
Changes in the cornea are insignificant - punctate epithelial infiltrates that disappear without a trace.
Treatment consists in the use of antiviral eye drops (interferon, interferon inducers) in combination with anti-inflammatory drugs (first antiallergic, and from the 2nd week of corticosteroids). Duration of treatment is 9-14 days. Recovery is usually without consequences.
Herpesvirus conjunctivitis.
Although herpetic eye lesions are among the most common diseases, and herpetic keratitis is recognized as the most common corneal lesion in the world, herpesvirus conjunctivitis is most often a component of primary infection with the herpes virus in early childhood.
Primary herpetic conjunctivitis more often has a follicular nature, as a result of which it is difficult to distinguish it from adenoviral. For herpetic conjunctivitis, the following symptoms are characteristic: one eye is affected, the edges of the eyelids, skin and cornea are often involved in the pathological process.
Recurrence of herpes can occur as follicular or vesicular-ulcerative conjunctivitis, but usually develops as superficial or deep keratitis (stromal, ulcerative, keratouveitis).
Antiviral treatment... Preference should be given to selective antiherpetic agents. Zovirax eye ointment is prescribed, which is applied 5 times in the first days and 3-4 times in subsequent days, or drops of interferon or an interferon inducer (instillations 6-8 times a day). Inside take Valtrex 1 tablet 2 times a day for 5 days or Zovirax 1 tablet 5 times a day for 5 days. Additional therapy: with moderate allergies - antiallergic drops alomid or lecrolin (2 times a day), with severe allergies - allergophthal or spersallerg (2 times a day). In case of damage to the cornea, drops of Vitasik, carnosine, taufon or korneregel are additionally installed 2 times a day; in case of a recurrent course, immunotherapy is carried out: Licopid, 1 tablet 2 times a day for 10 days. Immunotherapy with lycopid helps to increase the effectiveness of specific treatment of various forms of ophthalmic herpes and to significantly reduce the frequency of relapses.
Chlamydial eye diseases
Chlamydia(Chlamydia trachomatis) - an independent type of microorganisms; they are intracellular bacteria with a unique developmental cycle that exhibit the properties of viruses and bacteria. Different serotypes of chlamydia cause three different conjunctival diseases: trachoma (serotypes A-C), chlamydial conjunctivitis of adults and newborns (serotypes D-K), and lymphogranulomatosis venereal disease (serotypes L1, L2, L3).
Trachoma ... Trachoma is a chronic infectious keratoconjunctivitis characterized by the appearance of follicles with their subsequent scarring and papillae on the conjunctiva, inflammation of the cornea (pannus), and in the later stages - deformation of the eyelids. The emergence and spread of trachoma is associated with a low level of sanitary culture and hygiene. In economically developed countries, trachoma is practically not found. Huge work on the development and implementation of scientific, organizational and treatment-and-prophylactic measures led to the elimination of trachoma in our country. At the same time, according to WHO, trachoma remains the leading cause of blindness in the world. It is believed that active trachoma affects up to 150 million people, mainly in Africa, the Middle East and Asia. Trachoma infection in Europeans visiting these regions is still possible today.
Trachoma occurs as a result of the introduction of infectious agents into the conjunctiva of the eye. The incubation period is 7-14 days. The defeat is usually bilateral.
In the clinical course of trachoma, there are 4 stages. 
With a severe form and prolonged course of trachoma, corneal pannus- Infiltration extending to the upper segment of the cornea with vessels growing into it (Fig. 9.5).
Rice. 9.5. Trachomatous pannus.
Pannus is a characteristic feature of trachoma and is important in differential diagnosis. During the period of scarring at the site of the pannus, there is an intense opacity of the cornea in the upper half with decreased vision.
With trachoma, various complications from the eye and the adnexa can occur. The attachment of bacterial pathogens aggravates the inflammatory process and complicates the diagnosis. A serious complication is inflammation of the lacrimal gland, lacrimal ducts and lacrimal sac... The resulting purulent ulcers during trachoma, caused by a concomitant infection, are difficult to heal and can lead to perforation of the cornea with the development of inflammation in the eye cavity, and therefore there is a threat of eye death.
In the process of scarring, severe consequences of trachoma: shortening of the conjunctival vaults, the formation of adhesions of the eyelid with the eyeball (simblefaron), degeneration of the lacrimal and meibomian glands, causing xerosis of the cornea. Scarring causes cartilage curvature, eyelid curvature, and incorrect position of the eyelashes (trichiasis). In this case, the eyelashes touch the cornea, which leads to damage to its surface and contributes to the development of corneal ulcers. Narrowing of the lacrimal passages and inflammation of the lacrimal sac (dacryocystitis) can be accompanied by persistent lacrimation.
Laboratory diagnostics includes cytological examination of scrapings from the conjunctiva in order to detect intracellular inclusions, isolation of pathogens, and determination of antibodies in blood serum.
The main place in the treatment is occupied by antibiotics(tetracycline or erythromycin ointment), which are used according to two main schemes: 1-2 times a day for mass treatment or 4 times a day for individual therapy, respectively, for several months to several weeks. The expression of follicles with special tweezers to increase the effectiveness of therapy is currently practically not used. Trichiasis and volvulus of the eyelids are surgically removed. The prognosis with timely treatment is favorable. Relapses are possible, therefore, after completing the course of treatment, the patient should be monitored for a long period of time.
Chlamydial conjunctivitis ... There are chlamydial conjunctivitis (paratrachoma) of adults and newborns. Epidemic chlamydial conjunctivitis in children, chlamydial uveitis, chlamydial conjunctivitis in Reiter's syndrome are much less common.
Chlamydial conjunctivitis in adults- infectious subacute or chronic infectious conjunctivitis caused by C. trachomatis and sexually transmitted infections. The prevalence of chlamydial conjunctivitis in developed countries is slowly but steadily growing; they make up 10-30% of the identified conjunctivitis. Infection usually occurs between the ages of 20-30. Women get sick 2-3 times more often. Conjunctivitis is mainly associated with urogenital chlamydial infection, which may be asymptomatic.
The disease is characterized by an inflammatory reaction of the conjunctiva with the formation of numerous follicles that are not prone to scarring. More often one eye is affected, a bilateral process is observed in about 1/3 of patients. The incubation period is 5-14 days. Conjunctivitis more often (in 65% of patients) occurs in an acute form, less often (in 35%) - in a chronic one.
Clinical picture: pronounced edema of the eyelids and narrowing of the palpebral fissure, severe hyperemia, edema and infiltration of the conjunctiva of the eyelids and transitional folds. Particularly characteristic are large loose follicles located in the lower transitional fold and subsequently merging in the form of 2-3 ridges. Discharged at first mucopurulent, in small quantities, with the development of the disease, it becomes purulent and abundant. In more than half of the patients, a slit lamp study reveals lesions of the upper limb in the form of edema, infiltration and vascularization. Often, especially in the acute period, there is a lesion of the cornea in the form of superficial punctate infiltrates that are not stained with fluorescein. From the 3-5th day of the disease on the side of the lesion, regional preauricular adenopathy occurs, as a rule, painless. Often, on the same side, the phenomena of Eustachitis are noted: noise and pain in the ear, hearing loss.
Treatment: ocacin eye drops 6 times a day or tetracycline, erythromycin ophthalmic ointment, "..." 5 times a day, from the 2nd week drops 4 times, ointment 3 times, inside - antibiotic tavanik, 1 tablet a day for 5-10 days. Additional therapy includes instillation of antiallergic drops: in the acute period - allergophthal or spersallerga 2 times a day, in the chronic - alomide or lecrolin 2 times a day, inside - antihistamines for 5 days. From the 2nd week, dexapos or maxidex eye drops are prescribed once a day.
Epidemic chlamydial conjunctivitis ... The disease is more benign than paratrachoma, and occurs in the form of outbreaks in visitors to baths, swimming pools and children 3-5 years old in organized groups (orphanages and children's homes). The disease can begin acutely, subacutely, or proceed as a chronic process.
Usually one eye is affected: hyperemia, edema, infiltration of the conjunctiva, papillary hypertrophy, follicles in the lower fornix are found. The cornea is rarely involved in the pathological process; reveal point erosion, subepithelial point infiltrates. A slight preauricular adenopathy is often found.
All conjunctival phenomena and without treatment can undergo a reverse development after 3-4 weeks. Local treatment: tetracycline, erythromycin or "..." ointment 4 times a day or ocacin eye drops or "..." 6 times a day.
Chlamydial conjunctivitis (paratrachoma) of newborns ... The disease is associated with urogenital chlamydial infection: it is detected in 20-50% of children born from mothers infected with chlamydia. The incidence of chlamydial conjunctivitis reaches 40% of all neonatal conjunctivitis.
Is of great importance preventive eye treatment in newborns, which, however, is difficult due to the lack of highly effective, reliable means, since the traditionally used solution of silver nitrate does not prevent the development of chlamydial conjunctivitis. Moreover, his instillations often cause irritation of the conjunctiva, that is, contribute to the onset of toxic conjunctivitis.
Clinically, chlamydial conjunctivitis of newborns proceeds as acute papillary and subacute infiltrative conjunctivitis.
The disease begins acutely on the 5-10th day after childbirth with the appearance of an abundant liquid purulent discharge, which, due to an admixture of blood, may have a brown tint. Edema of the eyelids is sharply expressed, the conjunctiva is hyperemic, edematous, with papillary hyperplasia, pseudomembranes can form. Inflammation subsides in 1-2 weeks. If active inflammation lasts more than 4 weeks, follicles appear, mainly on the lower eyelids. In about 70% of newborns, the disease develops in one eye. Conjunctivitis can be accompanied by preauricular adenopathy, otitis media, nasopharyngitis, and even chlamydial pneumonia.
Treatment: tetracycline or erythromycin ointment 4 times a day.
WHO (1986) gives the following recommendations for eye treatment for the prevention of conjunctivitis in newborns: in areas of increased risk of infection with gonococcal infection (most developing countries), instillations of 1% silver nitrate solution are prescribed, you can also lay 1% tetracycline ointment behind the eyelid. In areas of low risk of contracting gonococcal infection, but a high prevalence of chlamydia (most industrialized countries), they practice laying 1% tetracycline or 0.5% erythromycin ointment.
In the prevention of conjunctivitis in newborns, timely treatment of urogenital infections in pregnant women is central.
Allergic conjunctivitis
Allergic conjunctivitis- this is an inflammatory reaction of the conjunctiva to the effects of allergens, characterized by hyperemia and edema of the mucous membrane of the eyelids, edema and itching of the eyelids, the formation of follicles or papillae on the conjunctiva; sometimes accompanied by damage to the cornea with visual impairment.
Allergic conjunctivitis occupies an important place in the group of diseases, united by the general name "red eye syndrome": they affect about 15% of the population.
Due to the anatomical position of the eyes, they are often exposed to various allergens. Hypersensitivity often manifests itself in an inflammatory reaction of the conjunctiva (allergic conjunctivitis), but any part of the eye can be affected, and then allergic dermatitis and edema of the eyelid skin, allergic blepharitis, conjunctivitis, keratitis, iritis, iridocyclitis, retinitis, optic neuritis develop.
The eyes can be the site of the development of an allergic reaction in many systemic immunological disorders, and eye damage is often the most dramatic manifestation of the disease. An allergic reaction plays an important role in the clinical picture of eye infections.
Allergic conjunctivitis often combined with such systemic allergic diseases like bronchial asthma, allergic rhinitis, atopic dermatitis.
Hypersensitivity reactions(a synonym for allergies) are classified as immediate (developing within 30 minutes from the moment of exposure to the allergen) and delayed (developing 24-48 hours or later after exposure). This division of allergic reactions is of practical importance in the construction of pharmacotherapy. Immediate reactions are caused by a "friendly" release in the tissue at a certain site (local process) of biologically active mediators from granules of mast cells of the mucous membranes and blood basophils, which is called activation or degranulation of mast cells and basophils.
In some cases, the typical picture of the disease or its clear connection with the effects of an external allergenic factor leaves no doubt about the diagnosis. In most cases, the diagnosis of allergic eye diseases is associated with great difficulties and requires the use of specific allergological research methods.
Allergic history is the most important diagnostic factor. It should reflect data on hereditary allergic burden, features of the course of the disease, a set of effects that can cause an allergic reaction, the frequency and seasonality of exacerbations, the presence of allergic reactions, in addition to eye reactions. Naturally occurring or specially conducted elimination and exposure tests are of great diagnostic value. The first is to "turn off" the alleged allergen, the second - in the repeated exposure to them after the clinical phenomena subsided. Carefully collected anamnesis suggests a "guilty" allergenic agent in more than 70% of patients.
Skin allergy tests used in ophthalmic practice (application, prick-test, scarification, scarification-application), are low-traumatic and at the same time quite reliable.
Provocative allergic tests(conjunctival, nasal and sublingual) are used only in exceptional cases and with great caution.
Laboratory allergy diagnostics highly specific and possible in the acute period of the disease without fear of causing harm to the patient.
The identification of eosinophils in the co-brace from the conjunctiva is of great diagnostic value.
Basic principles of therapy:
- elimination, ie, exclusion, of the "guilty" allergen, if possible, is the most effective and safe method of preventing and treating allergic conjunctivitis;
- drug symptomatic therapy: local, with the use of ophthalmic drugs, and general - antihistamines inside with severe lesions occupy the main place in the treatment of allergic conjunctivitis;
- specific immunotherapy is carried out in medical institutions with insufficient effectiveness of drug therapy and the impossibility of excluding the "guilty" allergen.
For antiallergic therapy, two groups of eye drops are used: the first - inhibiting the degranulation of mast cells: cromones - 2% lecrolin solution, 2% lecrolin solution without preservative, 4% kuzikrom solution and 0.1% lodoxamide solution (alomid), the second is antihistamines: antazoline + tetrizoline (spersallerg) and antazolin + naphazoline (allergophthal). Additionally, corticosteroid drugs are used: 0.1% dexamethasone solution (dexapos, maxidex, oftan-dexamethasone) and 1% or 2.5% hydrocortisone-POS solution, as well as non-steroidal anti-inflammatory drugs - 1% diclofenac solution (naklof).
The following clinical forms of allergic conjunctivitis are most common, characterized by their own characteristics in the choice of treatment:
- pollinous conjunctivitis,
- vernal keratoconjunctivitis,
- drug allergy,
- chronic allergic conjunctivitis,
- large papillary conjunctivitis.
Pollinous conjunctivitis ... These are seasonal allergic eye diseases caused by pollen during the flowering period of grasses, cereals, and trees. The aggravation time is closely related to the pollination calendar of plants in each climatic region. Pollinous conjunctivitis can begin acutely: unbearable itching of the eyelids, burning under the eyelids, photophobia, lacrimation, edema and hyperemia of the conjunctiva. Conjunctival edema can be so severe that the cornea "sinks" into the surrounding chemotic conjunctiva. In such cases, marginal infiltrates appear in the cornea, more often in the region of the palpebral fissure. Semi-transparent focal superficial infiltrates located along the limbus can merge and ulcerate, forming superficial corneal erosion. More often, pollinous conjunctivitis occurs chronically with moderate burning sensation under the eyelids, slight discharge, recurrent itching of the eyelids, mild conjunctival hyperemia, small follicles or papillae on the mucous membrane can be found.
Treatment for chronic course: alomid or lecrolin 2 times a day for 2-3 weeks, in acute course - allergophthal or spersallerg 2-3 times a day. Additional therapy for severe cases: antihistamines by mouth for 10 days. For blepharitis, hydrocortisone-POS ointment is applied to the eyelids. In case of persistent recurrent course, specific immunotherapy is carried out under the supervision of an allergist.
Spring keratoconjunctivitis (spring catarrh) ... The disease usually occurs in children aged 3-7 years, more often in boys, has a predominantly chronic persistent debilitating course. The clinical manifestations and prevalence of spring catarrh vary in different areas. The most characteristic clinical sign is papillary growths on the conjunctiva of the upper eyelid cartilage (conjunctival form), usually small, flattened, but can be large, deforming the eyelid (Fig. 9.6).

Rice. 9.6. Spring keratoconjunctivitis.
Less commonly, papillary growths are located along the limbus (limbal form). Sometimes there is a mixed form. The cornea is often affected: epitheliopathy, erosion or corneal ulcer, keratitis, hyperkeratosis.
Treatment: in case of mild course, instillation of alomid or lecrolin is performed 3 times a day for 3-4 weeks. In severe cases, spersallerg or allergophthal is used 2 times a day. In the treatment of spring catarrh, a combination of antiallergic drops with corticosteroids is necessary: instillation of dexapos, maxidex or ophtan-dexamethasone eye drops 2-3 times a day for 3-4 weeks. Additionally, antihistamines (diazolin, suprastin or claritin) are prescribed orally for 10 days. For corneal ulcers, reparative agents (Vitasik Taufon eye drops or Solcoseryl, Corneregel gels) are used 2 times a day until the condition of the cornea improves5. With a long, persistent course of spring catarrh, a course of treatment with histoglobulin (4-10 injections) is carried out.
Drug allergic conjunctivitis ... The disease can occur acutely after the first use of any medicine, but usually develops chronically with prolonged treatment with the drug, and an allergic reaction to both the main medicine and the preservative of the eye drops is possible. An acute reaction occurs within 1 hour after drug administration (acute drug conjunctivitis, anaphylactic shock, acute urticaria, Quincke's edema, systemic capillary toxicosis, etc.). A subacute reaction develops during the day (Fig. 9.7).

Rice. 9.7. Medicinal blepharoconjunctivitis (subacute).
A lingering reaction occurs over several days and weeks, usually with prolonged topical administration of drugs. Eye reactions of the latter type are most common (in 90% of patients) and are chronic. Almost any drug can cause an allergic reaction in the eye. The same drug can cause different manifestations in different patients. However, different drugs can cause a similar clinical picture of drug allergy.
The characteristic signs of acute allergic inflammation are hyperemia, edema of the eyelids and conjunctiva, lacrimation, sometimes hemorrhage; chronic inflammation is characterized by itching of the eyelids, hyperemia of the mucous membrane, moderate discharge, and the formation of follicles. With drug allergy, the conjunctiva, cornea, eyelid skin are most often affected, much less often the choroid, retina, and optic nerve.
The main attraction of drug allergies is cancellation of the "guilty" drug or switching to the same drug without a preservative.
After the cancellation of the "guilty" drug in acute course, eye drops allergophthal or spersallerg are used 2-3 times a day, in chronic - alomid, lecrolin or lecrolin without preservative 2 times a day. With a severe and prolonged course, there may be a need to take antihistamines by mouth.
Chronic allergic conjunctivitis ... Allergic conjunctivitis is more often chronic: moderate burning of the eyes, slight discharge, recurrent itching of the eyelids. It should be borne in mind that often numerous complaints of discomfort are combined with minor clinical manifestations, which complicates the diagnosis.
Among the reasons for the persistent course may be increased sensitivity to pollen, industrial hazards, food products, household chemicals, house dust, dandruff and animal hair, dry fish food, medicines, cosmetics, contact lenses.
The most important treatment is exclusion of risk factors for the development of allergies, if they can be established. Local treatment includes instillation of eye drops of lecrolin or alomid 2 times a day for 3-4 weeks. When blepharitis occurs, hydrocortisone-POS eye ointment is prescribed 2 times a day for the eyelids and instillation of artificial tears (natural tears) 2 times a day.
Allergic conjunctivitis while wearing contact lenses ... It is believed that most patients wearing contact lenses will someday have an allergic reaction of the conjunctiva: eye irritation, photophobia, lacrimation, burning under the eyelids, itching, discomfort when inserting the lens. On examination, you can find small follicles, small or large papillae on the conjunctiva of the upper eyelids, hyperemia of the mucous membrane, edema and pinpoint erosion of the cornea.
Treatment: it is necessary to refuse to wear contact lenses. Prescribe the instillation of eye drops of lecrolin or alomid 2 times a day. In case of an acute reaction, allergophthal or spersallerg is used 2 times a day.
Large papillary conjunctivitis (CPC) ... The disease is an inflammatory reaction of the conjunctiva of the upper eyelid, which has been in contact with a foreign body for a long period. The emergence of PDA is possible under the following conditions: wearing contact lenses (hard and soft), the use of eye prostheses, the presence of sutures after cataract extraction or keratoplasty, tightening scleral fillings.
Patients complain of itching and mucous discharge. In severe cases, ptosis may occur. Large (giant - with a diameter of 1 mm or more) papillae are grouped over the entire surface of the conjunctiva of the upper eyelids.
Although the clinical picture of CPC is very similar to the manifestations of the conjunctival form of spring catarrh, there are significant differences between them. First of all, the PDA develops at any age. and is mandatory if there are remaining stitches or wearing contact lenses. Complaints of itching and discharge with PDA are less pronounced, the limbus and cornea are usually not involved in the process. Finally, all symptoms of CPC quickly disappear after removal of the foreign body. Patients with CPC do not necessarily have a history of allergic diseases and seasonal exacerbations are not observed.
In treatment, the main importance is foreign body removal... Until the symptoms disappear completely, alomid or lecrolin is instilled 2 times a day. Wearing new contact lenses is possible only after the inflammatory phenomena have completely disappeared. For the prevention of PDA, systematic care of contact lenses and prostheses is required.
Prevention of allergic conjunctivitis... In order to prevent the disease, certain measures must be taken.
- Elimination of causal factors. It is important to reduce, and if possible, exclude contact with such risk factors for the development of allergies as house dust, cockroaches, pets, dry fish food, household chemicals, cosmetics. It should be remembered that in patients with allergies, eye drops and ointments (especially antibiotics and antiviral agents) can cause not only allergic conjunctivitis, but also a general reaction in the form of urticaria and dermatitis.
- In the event that it is assumed that a person will get into such conditions when it is impossible to exclude contact with factors causing allergies to which he is sensitive, one drop of lecroline or alomide should be started, one drop 1-2 times a day, 2 weeks before contact.
- If the patient has already got into such conditions, allergophthal or spersallerg is instilled, which give an immediate effect that lasts for 12 hours.
- With frequent relapses, specific immunotherapy is performed during the period of conjunctivitis remission.
Dystrophic diseases of the conjunctiva
This group of conjunctival lesions includes several diseases of various origins:
- keratoconjunctivitis dry,
- pinguecula,
- pterygoid hymen.
Dry eye syndrome (keratoconjunctivitis dry) - This is a lesion of the conjunctiva and cornea, which occurs in connection with a pronounced decrease in the production of tear fluid and a violation of the stability of the tear film.
The tear film consists of three layers. The superficial, lipid layer produced by the meibomian glands prevents the evaporation of fluid, thereby maintaining the stability of the lacrimal meniscus. The middle, aqueous, layer, which makes up 90% of the thickness of the tear film, is formed by the main and accessory lacrimal glands. The third layer, directly covering the corneal epithelium, is a thin mucin film produced by the goblet cells of the conjunctiva. Each layer of the tear film can be affected by various diseases, hormonal disorders, medicinal effects, which leads to the development of keratoconjunctivitis dry.
Dry eye syndrome is a widespread disease, especially in people over 70 years of age.
Patients complain about sensation of a foreign body under the eyelids, burning, stinging, dryness in the eye, photophobia, poor wind and smoke tolerance are noted. All phenomena worsen in the evening. Eye irritation is caused by instillation of any eye drops. Objectively, dilated vessels of the scleral conjunctiva, a tendency to the formation of folds of the mucous membrane, flocculent inclusions in the lacrimal fluid, and the surface of the cornea dull. The following clinical forms of corneal lesions are distinguished, corresponding to the severity of the disease: epitheliopathy (barely noticeable or punctate defects of the corneal epithelium, detected by staining with fluorescein or rose Bengal), corneal erosion (more extensive epithelial defects), filamentous keratitis (epithelial flaps of filaments, twisted in the form one end fixed to the cornea), corneal ulcer.
When diagnosing dry eye syndrome, the characteristic complaints of the patient are taken into account, the results of biomicroscopic examination of the edges of the eyelids, conjunctiva and cornea, as well as special tests.
- Test for assessing the stability of the tear film (test according to Norn). When looking down, with the upper eyelid pulled back, a 0.1-0.2% solution of fluorescein is instilled into the limbus area at 12 o'clock. After turning on the slit lamp, the patient should not blink. Observing the painted surface of the tear film, the time of the film rupture (black spot) is determined. The tear film rupture time of less than 10 s is of diagnostic value.
- Schirmer's test with a standard strip of filter paper, one end inserted in the lower eyelid. After 5 minutes, the strip is removed and the length of the wetted part is measured: its value less than 10 mm indicates a slight decrease in the production of tear fluid, and less than 5 mm - about a significant one.
- A test with a 1% solution of Rose Bengal is especially informative, as it allows you to identify dead (stained) cells of the epithelium covering the cornea and conjunctiva.
Diagnosis of dry eye syndrome is associated with great difficulties and is based only on the results of a comprehensive assessment of the patient's complaints and the clinical picture, as well as the results of functional tests.
Treatment remains a difficult task and involves the gradual individual selection of medicines. Eye drops containing a preservative are less tolerated by patients and can cause an allergic reaction, so preference should be given to eye drops without a preservative. The main place is occupied by means of tear replacement therapy. Natural tear drops are used 3-8 times a day, and Oftagel or Vidisic-gel gel compositions are used 2-4 times a day. In case of allergic irritation of the conjunctiva, add alomid, lecrolin or lecrolin without preservative (2 times a day for 2-3 weeks). In case of damage to the cornea, vitasik drops, carnosine, taufon or solcoseryl gel or corneregel are used.
Pinguecula (wen) - This is an elastic formation of an irregular shape slightly rising above the conjunctiva, located a few millimeters from the limbus within the palpebral fissure on the nasal or temporal side. Usually occurs in older people symmetrically in both eyes. Pinguecula does not cause painful sensations, although it attracts the patient's attention. No treatment is required, except in rare cases when Pinguecula becomes inflamed. In this case, anti-inflammatory eye drops (dexapos, maxidex, oftan-dexamethasone or hydrocortisone-POS) are used, and when pinguecula is combined with a mild secondary bacterial infection, complex preparations (dexagentamicin or maxitrol) are used.
Pterygoid hymen (pterygium) - a flat superficial vascularized fold of the conjunctiva of a triangular shape, growing on the cornea. Irritation factors, wind, dust, temperature changes can stimulate the growth of pterygium, which leads to visual impairment. The pterygium slowly moves towards the center of the cornea, tightly connects with the Bowman's membrane and the superficial layers of the stroma. To delay the growth of pterygium and prevent relapse, anti-inflammatory and antiallergic drugs are used (drops of alomid, lecrolin, dexapos, maxidex, oftan-dexamethasone, hydrocortisone-POS or naklof). Surgical treatment should be carried out during a period when the film has not yet covered the central part of the cornea. When the recurrent pterygium is excised, a marginal layer-by-layer keratoplasty is performed.
Article from the book:.
The disease cannot adapt to the knowledge of the doctor.
Paracelsus
9.1. The structure and function of the conjunctiva
The conjunctiva, or conjunctiva, is the mucous membrane that lines the back of the eyelids and extends to the eyeball all the way to the cornea and thus connects the eyelid to the eyeball. When the palpebral fissure is closed, the connective membrane forms a closed cavity - the conjunctival sac, which is a narrow slit-like space between the eyelids and the eyeball.
The mucous membrane that covers the back of the eyelids is called the conjunctiva of the eyelids, and the overlying sclera is called the conjunctiva of the eyeball or sclera. The part of the conjunctiva of the eyelids, which, forming the vaults, passes to the sclera, is called the conjunctiva of the transitional folds or the vault. Accordingly, the upper and lower conjunctival vaults are distinguished. At the inner corner of the eye, in the region of the third eyelid rudiment, the conjunctiva forms a vertical semilunar fold and a lacrimal meatus.
In the conjunctiva, two layers are distinguished - epithelial and subepithelial. The conjunctiva of the eyelids is tightly fused with the cartilaginous plate. The epithelium of the conjunctiva is multilayered, cylindrical, with a large number of goblet cells. The conjunctiva of the eyelids is smooth, shiny, pale pink, through it
The yellowish columns of the meibomian glands passing through the thickness of the cartilage are visible. Even with the normal state of the mucous membrane at the outer and inner corners of the eyelids, the conjunctiva covering them looks slightly hyperemic and velvety due to the presence of small papillae.
The conjunctiva of the transitional folds is loosely connected to the underlying tissue and forms folds that allow the eyeball to move freely. The fornix conjunctiva is covered with stratified squamous epithelium with a small number of goblet cells. The subepithelial layer is represented by loose connective tissue with inclusions of adenoid elements and accumulations of lymphoid cells. Numerous mast cells of the conjunctiva determine the allergic reaction of the mucous membrane. The conjunctiva contains a large number of Krause lacrimal glands.
The conjunctiva of the sclera is tender, loosely connected to the episcleral tissue. The stratified squamous epithelium of the conjunctiva of the sclera smoothly passes onto the cornea.
The conjunctiva borders on the skin of the edges of the eyelids, and on the other hand, on the corneal epithelium. Diseases of the skin and cornea can spread to the conjunctiva, while diseases of the conjunctiva can spread to the skin of the eyelids (blepharoconjunctivitis) and the cornea (keratoconjunctivitis). Through the lacrimal opening and the lacrimal canal, the conjunctiva is also connected with the mucous membrane of the lacrimal sac and nose.
The conjunctiva is abundantly supplied with blood from the arterial branches of the eyelids, as well as from the anterior ciliary vessels. Any inflammation and irritation of the mucous membrane is accompanied by a bright hyperemia of the vessels of the conjunctiva of the eyelids and vaults, the intensity of which decreases towards the limbus.
Due to the dense network of nerve endings of the first and second branches of the trigeminal nerve, the conjunctiva plays the role of integumentary sensitive epithelium.
The main physiological function of the conjunctiva is to protect the eye: when a foreign body enters, irritation of the eye appears, the secretion of lacrimal fluid increases, blinking movements become more frequent, as a result of which the foreign body is mechanically removed from the conjunctival cavity. The secret of the conjunctival sac constantly wets the surface of the eyeball, reduces friction during its movements, and helps to preserve the transparency of the moist cornea. This secret is rich in protective elements: immunoglobulins, lysozyme, lactoferrin. The protective role of the conjunctiva is also ensured by the abundance of lymphocytes, plasma cells, neutrophils, mast cells and the presence of immunoglobulins of all five classes (see section 3.3.2).
9.2. Diseases of the conjunctiva
Among the diseases of the conjunctiva, the main place is occupied by inflammatory diseases. Conjunctivitis is an inflammatory reaction of the conjunctiva to various influences, characterized by hyperemia and edema of the mucous membrane; swelling and itching of the eyelids, separated from the conjunctiva, the formation of follicles or papillae on it; sometimes accompanied by damage to the cornea with visual impairment.
Conjunctival hyperemia is an alarming signal common to many eye diseases (acute iritis, an attack of glaucoma, an ulcer or corneal injury, scleritis, episcleritis), therefore, when establishing a diagnosis of conjunctivitis, it is necessary to exclude other diseases accompanied by eye redness.
The following three groups of conjunctival diseases have fundamental differences:
Infectious conjunctivitis (bacterial, viral, chlamydial);
Allergic conjunctivitis (hay fever, spring catarrh, drug allergy, chronic allergic conjunctivitis, large papillary conjunctivitis, atopic blepharoconjunctivitis);
Dystrophic diseases of the conjunctiva (keratoconjunctivitis dry, pinguecula, pterygium).
9.2.1. Infectious conjunctivitis
9.2.1.1. Bacterial conjunctivitis
Any of the widespread pathogens of a purulent infection can cause inflammation of the conjunctiva. Cocci, especially staphylococci, are the most common cause of conjunctival infection, but it proceeds more favorably. The most dangerous pathogens are Pseudomonas aeruginosa and gonococcus, which cause severe acute conjunctivitis, in which the cornea is often affected (Fig. 9.1).
Acute and chronic conjunctivitis caused by staphylococcus. Acute conjunctivitis occurs more often in children, less often in the elderly, and even less often in people of average
Rice. 9.1. Acute bacterial conjunctivitis.
age. Usually, the pathogen enters the eye from the hands. First, one eye is affected, after 2-3 days the other. The clinical manifestations of acute conjunctivitis are as follows. In the morning, the patient can hardly open his eyes, as the eyelids stick together. When the conjunctiva is irritated, the amount of mucus increases. The nature of the discharge can rapidly change from mucous to mucopurulent and purulent. The discharge drains over the edge of the eyelid, dries up on the eyelashes. External examination reveals hyperemia of the conjunctiva of the eyelids, transitional folds and sclera. The mucous membrane swells, loses its transparency, the pattern of the meibomian glands is erased. The severity of superficial conjunctival vascular infection decreases towards the cornea. The patient is worried about discharge on the eyelids, itching, burning sensation and photophobia.
Chronic conjunctivitis develops slowly, proceeds with periods of improvement. Patients are worried about photophobia, mild irritation and rapid eye fatigue. The conjunctiva is moderately hyperemic, loosened, along the edge of the eyelids, dried
mine (crust). Conjunctivitis can be associated with nasopharyngeal disease, otitis media, sinusitis. In adults, conjunctivitis often occurs with chronic blepharitis, dry eye syndrome, damage to the lacrimal duct.
To identify a bacterial infection in conjunctivitis of newborns and acute conjunctivitis, microscopic examination of smears and cultures of discharge from the conjunctiva is used. The isolated microflora is examined for pathogenicity and sensitivity to antibiotics.
In the treatment, the main place is occupied by local antibacterial therapy: sodium sulfacyl, vitabact, fucitalmic are instilled 3-4 times a day or an eye ointment is applied: tetracycline, erythromycin, floxal 2-3 times a day. In acute course, eye drops are prescribed: tobrex, tobrex 2X, cypromed, lofox, uniflox or floxal up to 4-6 times a day. In case of edema and severe irritation of the conjunctiva, instillations of antiallergic or anti-inflammatory drops (opatanol, zaditen, lecrolin or indocollir) are added 2 times a day.
In acute conjunctivitis, it is impossible to tie and glue the eye, since under the bandage favorable conditions are created for the multiplication of bacteria, the threat of corneal inflammation increases.
Acute conjunctivitis caused by Pseudomonas aeruginosa. The disease begins acutely: there is a large or moderate amount of purulent discharge and edema of the eyelids, the conjunctiva of the eyelids is sharply hyperemic, bright red, edematous, loosened. Without treatment, conjunctival infection can easily spread to the cornea and cause a rapidly progressive ulcer to form.
Treatment: instillation of antibacterial eye drops (tobrex,
tobrex 2X, lofox, cypromed, floxal or gentamicin) in the first 2 days 6-8 times a day, then up to 3-4. The most effective combination of two antibiotics, for example, Tobrex + Cypromed or Gentamicin + Polymyxin. When the infection spreads to the cornea, tobramycin, gentamicin or ceftazidime are injected parabulbar and tavanic in tablets or gentamicin, tobramycin in the form of injections are systemically used. With pronounced edema of the eyelids and conjunctiva, antiallergic and anti-inflammatory drops are additionally instilled
(spersallerg, allergophthal or naklof) 2 times a day. In case of damage to the cornea, metabolic therapy means are needed - drops (taufon, vitasik, carnosine) or gels (corneregel, solcoseryl).
Acute conjunctivitis caused by gonococcus. Sexually transmitted disease (direct genital-eye contact or genital-hand-eye transmission). Hyperactive purulent conjunctivitis is characterized by rapid progression. The eyelids are edematous, the discharge is profuse, purulent, the conjunctiva is sharply hyperemic, bright red, irritated, gathers in protruding folds, often there is edema of the scleral conjunctiva (chemosis). Keratitis develops in 15-40% of cases, at first superficial, then a corneal ulcer forms, which can lead to perforation in 1-2 days.
In acute conjunctivitis, presumably caused by Pseudomonas aeruginosa or gonococcus, treatment is started immediately, without waiting for laboratory confirmation, since a delay of 1-2 days can lead to the development of corneal ulcers and eye death.
Treatment: with gonococcal conjunctivitis, laboratory confirmed or suspected on the basis of clinical manifestations
and anamnesis of the disease, antibacterial therapy is first carried out: rinsing the eye with a solution of boric acid, instillation of eye drops (cypromed, floxal or penicillin) 6-8 times a day. Systemic treatment is carried out: quinolone antibiotic 1 tablet 2 times a day or intramuscular penicillin. Additionally, instillations of antiallergic or anti-inflammatory drugs (polynadym, opatanol or diclo-F) are prescribed 2 times a day. With the symptoms of keratitis, Vitasik or Taufon is also instilled 2 times a day.
Of particular danger is gonococcal conjunctivitis in newborns (gonoblenorrhea). Infection occurs during the passage of the fetus through the birth canal of a mother with gonorrhea. Conjunctivitis usually develops 2-5 days after birth. Swollen, dense, bluish-purple eyelids are almost impossible to open for examination of the eye. When pressed, bloody-purulent discharge is poured out of the palpebral fissure. The conjunctiva is sharply hyperemic, loosened, bleeds easily. The exclusive danger of gonoblenorrhea is damage to the cornea up to the death of the eye. Local treatment is the same as in adults, and systemic - the introduction of antibacterial drugs in doses corresponding to age.
Diphtheria conjunctivitis. Diphtheria of the conjunctiva, caused by a diphtheria bacillus, is characterized by the appearance on the conjunctiva of the eyelids with grayish films that are difficult to remove. The eyelids are dense, edematous. A cloudy liquid with flakes is released from the palpebral fissure. The films are tightly welded to the underlying tissue. Their separation is accompanied by bleeding, and after necrotization of the affected areas, scars are formed. The patient is isolated in the infectious diseases department and treated according to the diphtheria therapy regimen.
9.2.1.2. Viral conjunctivitis
Viral conjunctivitis is common and occurs in the form of epidemic outbreaks and episodic diseases.
Epidemic keratoconjunctivitis. Adenoviruses (more than 50 of their serotypes are already known) cause two clinical forms of eye damage: epidemic keratoconjunctivitis, which is more severe and accompanied by damage to the cornea, and adenoviral conjunctivitis, or pharyngoconjunctival fever.
Epidemic keratoconjunctivitis is a hospital-acquired infection, more than 70% of patients become infected in medical institutions. The source of infection is a patient with keratoconjunctivitis. The infection spreads by contact, less often by airborne droplets. Factors of transmission of the pathogen are infected hands of medical personnel, reusable eye drops, tools, devices, eye prostheses, contact lenses.
The duration of the incubation period of the disease is 3-14, more often 4-7 days. The duration of the infectious period is 14 days.
The onset of the disease is acute, usually both eyes are affected: first one, after 1-5 days the second. Patients complain of pain, sensation of a foreign body in the eye, lacrimation. The eyelids are edematous, the conjunctiva of the eyelids is moderately or significantly hyperemic, the lower transitional fold is infiltrated, folded, in most cases small follicles and punctate hemorrhages are revealed.
After 5-9 days from the onset of the disease, stage II of the disease develops, accompanied by the appearance of characteristic point infiltrates under the corneal epithelium. With the formation of a large number of infiltrates in the central zone of the cornea, vision decreases.
Regional adenopathy - an increase and soreness of the parotid lymph nodes - appears on the 1-2nd day of the disease in almost all patients. The defeat of the respiratory tract is observed in 5-25% of patients. The duration of epidemic keratoconjunctivitis is up to 3-4 weeks. A severe consequence of adenovirus infection is the development of dry eye syndrome due to impaired production of lacrimal fluid.
Laboratory diagnostics of acute viral conjunctivitis (adenoviral, herpetic) includes a method for determining fluorescent antibodies in conjunctival scrapings, polymerase chain reaction and, less often, a method for isolating the virus.
Treatment is difficult because there are no drugs selectively targeting adenoviruses. They use drugs with a broad antiviral effect: interferons (lokferon, ophthalmoferon, etc.) or interferon inducers, they are installed 6-8 times a day, and on the 2nd week, reducing their number to 3-4 times a day. In the acute period, the antiallergic drug Polynadim or Opatanol is additionally instilled 2-3 times a day and antihistamines are taken orally for 5-10 days. In cases of a subacute course, alomid drops or lecrolin are used 2 times a day. With a tendency to film formation and during the period of corneal eruptions, corticosteroids (dexapos, maxidex or ophtan-dexamethasone) are prescribed 2 times a day. For corneal lesions, taufon, vitasik or korneregel are used 2 times a day. In cases of a lack of tear fluid for a long period of time, tear substitutes are used: natural tear, ophtolic or chilo-chest of drawers 3-4 times a day, Oftagel or Vidisik-gel 2 times a day.
Prevention of nosocomial adenovirus infection includes the necessary anti-epidemic measures and sanitary and hygienic measures:
Examination of the eyes of each patient on the day of hospitalization to prevent the introduction of infection into the hospital;
Early detection of cases of development of diseases in a hospital;
Isolation of patients in isolated cases of disease and quarantine in outbreaks, anti-epidemic measures;
Sanitary and educational work.
Adenoviral conjunctivitis. The disease is milder than epidemic keratoconjunctivitis, and rarely causes outbreaks of nosocomial infection. The disease usually occurs in children's groups. The pathogen is transmitted by airborne droplets, less often by contact. The incubation period lasts 3-10 days.
The symptoms of the disease are similar to the initial clinical manifestations of epidemic keratoconjunctivitis, but their intensity is much lower: the discharge is scanty, the conjunctiva is hyperemic and moderately infiltrated, there are few follicles, they are small, sometimes there are punctate hemorrhages. In 1/2 of the patients, regional adenopathy of the parotid lymph nodes is found. Point epithelial infiltrates may appear on the cornea, but they disappear without a trace, without affecting visual acuity.
Adenoviral conjunctivitis is characterized by a general symptomatology: a lesion of the respiratory tract with an increase in body temperature and headache. Systemic damage may precede eye disease. Duration of adenoviral conjunctivitis 2 weeks.
Treatment includes instillation of interferons and antiallergic eye drops, and in case of insufficient lacrimal fluid, artificial tear preparations.
Prevention of nosocomial spread of infection is the same as in epidemic keratoconjunctivitis.
Epidemic hemorrhagic conjunctivitis (EGC). EGC, or acute hemorrhagic conjunctivitis, has been described relatively recently. The first EGC pandemic began in 1969 in West Africa and then spread to North Africa, the Middle East and Asia. The first EGC outbreak in Moscow was observed in 1971. Epidemic outbreaks in the world occurred in 1981-1984 and 1991-1992. The disease requires close attention, since EGC outbreaks in the world are repeated with a certain frequency.
The causative agent of EGC is enterovirus-70. EGC is characterized by a short incubation period, which is unusual for a viral disease - 12-48 hours. The main route of infection spread is contact. There is a high contagiousness of EGC, the epidemic is "explosive". In eye hospitals, in the absence of anti-epidemic measures, 80-90% of patients can be affected.
The clinical and epidemiological features of EGC are so characteristic that, on their basis, the disease can be easily distinguished from other ophthalmic infections. The onset is acute, first one eye is affected, after 8-24 hours - the second. Due to severe pain and photophobia, the patient seeks help on the first day. Mucous or mucopurulent discharge from the conjunctiva, the conjunctiva is sharply hyperemic, subconjunctival hemorrhages are especially characteristic: from point petechiae to extensive hemorrhages.

Rice. 9.2. Epidemic hemorrhagic conjunctivitis.
morrages, covering almost the entire conjunctiva of the sclera (Fig. 9.2). Changes in the cornea are insignificant - punctate epithelial infiltrates that disappear without a trace.
Treatment consists in the use of antiviral eye drops (interferon, interferon inducers) in combination with anti-inflammatory drugs (first antiallergic, and from the 2nd week of corticosteroids). Duration of treatment is 9-14 days. Recovery is usually without consequences.
Herpetic conjunctivitis.
Primary herpetic conjunctivitis often has the character of a rash of small vesicles that open up in the first hours, as a result of which it is difficult to distinguish it from other conjunctivitis. For herpetic conjunctivitis, the following symptoms are characteristic: one eye is affected, the edges of the eyelids, skin and cornea are often involved in the pathological process.
Recurrence of herpes can occur as vesicular-ulcerative conjunctivitis, but usually develops as superficial or deep keratitis (stromal, ulcerative, keratouveitis).
Antiviral treatment. Preference should be given to selective antiherpetic agents. Zovirax eye ointment is prescribed, which is applied 5 times in the first days and 3-4 times in subsequent days, or drops of ophthalmoferon or an interferon inducer (instillations 6-8 times a day). Inside take Valtrex 1 tablet 2 times a day for 5 days or Zovirax 1 tablet 5 times a day for 5 days. Additional therapy: with moderate allergies - anti-allergic drops zaditen or lecrolin (2 times a day), with severe allergies - polynadym or opatanol (2 times a day). In case of damage to the cornea, vitasik, taufon or korneregel drops are additionally instilled 2 times a day; in case of a recurrent course, immunotherapy is carried out: Licopid, 1 tablet 2 times a day for 10 days. Immunotherapy with lycopid helps to increase the effectiveness of specific treatment of various forms of ophthalmic herpes and to significantly reduce the frequency of relapses.
9.2.1.3. Chlomidial eye diseases
Chlamydia (Chlamydia trachomatis)- an independent type of microorganisms; they are intracellular bacteria with a unique developmental cycle that exhibit the properties of viruses and bacteria. Different serotypes of chlamydia cause three different conjunctival diseases: trachoma (serotypes A-C), chlamydial conjunctivitis of adults and newborns (serotypes D-K), and lymphogranulomatosis venereal disease (serotypes L1, L2, L3).
Trachoma. Trachoma is a chronic infectious keratoconjunctivitis characterized by the appearance of follicles with their subsequent scarring and papillae on the conjunctiva.
ve, inflammation of the cornea (pannus), and in the later stages - deformation of the eyelids. The emergence and spread of trachoma is associated with a low level of sanitary culture and hygiene. According to WHO, trachoma remains the main cause of blindness, mainly in Africa, the Middle East and Asia. Trachoma infection in Europeans visiting these regions is still possible today.
Trachoma occurs as a result of the introduction of infectious agents into the conjunctiva of the eye. The incubation period is 7-14 days. The defeat is usually bilateral.
In the clinical course of trachoma, there are 4 stages. IN Stage I there is an acute development of inflammatory reactions, diffuse infiltration, edema of the conjunctiva with the development of single follicles in it, which look like turbid gray grains located randomly and deeply. The formation of follicles on the conjunctiva of the upper cartilage is characteristic (Fig. 9.3). In Stage II against the background of increased infiltration and development of follicles, their disintegration begins, scars are formed, and corneal damage is pronounced. IN Stage III scarring processes prevail in the presence of follicles and infiltration. It is the formation of scars on the conjunctiva that makes it possible to distinguish trachoma from chlamydial conjunctivitis and other follicular conjunctivitis. IN Stage IV diffuse scarring of the affected mucous membrane occurs in the absence of inflammation in the conjunctiva and cornea (Fig. 9.4).
With a severe form and prolonged course of trachoma, corneal pannus may occur - infiltration extending to the upper segment of the cornea with vessels growing into it (Fig. 9.5). Pannus is a characteristic feature of trachoma and is important in differential diagnosis. During the scarring period on

Rice. 9.3. Trachoma, stage I.

Rice. 9.4. Trachoma, stage IV, cicatricial.

Rice. 9.5. Trachomatous pannus.
In the place of pannus, an intense opacity of the cornea occurs in the upper half with decreased vision.
With trachoma, various complications- damage to the eye and accessory apparatus.
The attachment of bacterial pathogens aggravates the inflammatory process and complicates the diagnosis. A serious complication is inflammation of the lacrimal gland, lacrimal tubules and lacrimal sac. Purulent ulcers formed during trachoma caused by concomitant infection are difficult to heal and can lead to corneal perforation with the development of inflammation in the eye cavity, and therefore there is a threat of eye death.
In the process of scarring, severe consequences trachoma: shortening of the conjunctival fornices, the formation of adhesions of the eyelid with the eyeball (simblefaron), degeneration of the lacrimal and meibomian glands, causing xerosis of the cornea. Scarring causes cartilage curvature, eyelid curvature, and incorrect position of the eyelashes (trichiasis). In this case, the eyelashes touch the cornea, which leads to damage to its surface and contributes to the development of corneal ulcers. Narrowing of the lacrimal passages and inflammation of the lacrimal sac (dacryocystitis) can be accompanied by persistent lacrimation.
Laboratory diagnostics includes cytological examination of scrapings from the conjunctiva in order to detect intracellular inclusions, isolation of pathogens, and determination of antibodies in blood serum.
The main place in the treatment is occupied by antibiotics (tetracycline or erythromycin ointment), which are used according to two main schemes: 1-2 times a day for mass treatment or 4 times a day for individual therapy, respectively, for several months to several weeks. The expression of follicles with special tweezers to increase the effectiveness of therapy is currently practically not used. Trichiasis and volvulus of the eyelids are surgically removed. Forecast for
timely treatment is favorable. Relapses are possible, therefore, after completing the course of treatment, the patient should be monitored for a long period of time.
Chlamydial conjunctivitis. There are chlamydial conjunctivitis (paratrachoma) of adults and newborns. Epidemic chlamydial conjunctivitis in children, chlamydial uveitis, chlamydial conjunctivitis in Reiter's syndrome are much less common.
Chlamydial conjunctivitis in adults - infectious subacute or chronic infectious conjunctivitis caused by C. trachomatis and sexually transmitted diseases. The prevalence of chlamydial conjunctivitis in developed countries is slowly but steadily growing. Infection usually occurs between the ages of 20-30. Conjunctivitis is mainly associated with urogenital chlamydial infection, which may be asymptomatic.
The disease is characterized by an inflammatory reaction of the conjunctiva with the formation of numerous follicles that are not prone to scarring. More often one eye is affected, a bilateral process is observed in about 1/3 of patients. The incubation period is 5-14 days. Conjunctivitis more often (in 65% of patients) occurs in an acute form, less often (in 35%) - in a chronic one.
Clinical picture: pronounced edema of the eyelids and narrowing of the palpebral fissure, severe hyperemia, edema and infiltration of the conjunctiva of the eyelids and transitional folds. Particularly characteristic are large loose follicles located in the lower transitional fold and subsequently merging in the form of 2-3 ridges. Discharged at first mucopurulent, in a small amount, with the development of the disease, it becomes purulent and profuse
nym. Often, especially in the acute period, there is a lesion of the cornea in the form of superficial small-point infiltrates that are not stained with fluorescein. From the 3-5th day of the disease on the side of the lesion, regional preauricular adenopathy occurs, as a rule, painless. Often, on the same side, the phenomena of Eustachitis are noted: noise and pain in the ear, hearing loss.
Treatment: eye drops cipromed or lofox 6 times a day or tetracycline, erythromycin, floxalic ointment 5 times a day, from the 2nd week drops 4 times, ointment 3 times, inside - antibiotic tavanik, 1 tablet a day for 5- 10 days. Additional therapy includes instillation of antiallergic drops: in the acute period - polynadym or opatanol 2 times a day, in the chronic - zaditen or lecrolin 2 times a day, inside - antihistamines for 5 days. From the 2nd week, dexapos or maxidex eye drops are prescribed once a day.
Epidemic chlamydial conjunctivitis. The disease is more benign than paratrachoma, and occurs in the form of outbreaks in visitors to baths, swimming pools and children 3-5 years old in organized groups (orphanages and children's homes). The disease can begin acutely, subacutely, or proceed as a chronic process. Usually one eye is affected: hyperemia, edema, infiltration of the conjunctiva, papillary hypertrophy, follicles in the lower fornix are found. The cornea is rarely involved in the pathological process; reveal point erosion, subepithelial point infiltrates. A slight preauricular adenopathy is often found.
All conjunctival phenomena and without treatment can undergo a reverse development after 3-4 weeks.
Local treatment: tetracycline, erythromycin or floxal ointment 4 times a day or cypromed or floxal eye drops 6 times a day.
Chlamydial conjunctivitis (paratrachoma) of newborns. The disease is associated with urogenital chlamydial infection of the mother.
Of great importance is the prophylactic treatment of the eyes in newborns, which, however, is difficult due to the lack of highly effective, reliable means, since the traditionally used silver nitrate solution does not prevent the development of chlamydial conjunctivitis. Moreover, his instillations often cause irritation of the conjunctiva, that is, contribute to the onset of toxic conjunctivitis.
Clinically, chlamydial conjunctivitis of newborns proceeds as acute papillary and subacute infiltrative conjunctivitis.
The disease begins acutely on the 5-10th day after childbirth with the appearance of an abundant liquid purulent discharge, which, due to an admixture of blood, may have a brown tint. Edema of the eyelids is sharply expressed, the conjunctiva is hyperemic, edematous, with papillary hyperplasia, pseudomembranes can form. Inflammation subsides in 1-2 weeks. If active inflammation lasts more than 4 weeks, follicles appear, mainly on the lower eyelids. Conjunctivitis can be accompanied by preauricular adenopathy, otitis media, nasopharyngitis, and even chlamydial pneumonia.
Treatment: tetracycline or erythromycin ointment 4 times a day.
countries) appoint instillations of a 1% solution of silver nitrate, you can also lay a 1% tetracycline ointment behind the eyelid. In areas of low risk of contracting gonococcal infection, but a high prevalence of chlamydia (most industrialized countries), they practice laying 1% tetracycline or 0.5% erythromycin ointment.
9.2.2. Allergic conjunctivitis
Allergic conjunctivitis- it is an inflammatory reaction of the conjunctiva to the effects of allergens, characterized by hyperemia and edema of the mucous membrane of the eyelids, edema and itching of the eyelids, the formation of follicles or papillae on the conjunctiva; sometimes accompanied by damage to the cornea with visual impairment.
Hypersensitivity often manifests itself in an inflammatory reaction of the conjunctiva (allergic conjunctivitis), but any part of the eye can be affected, and then allergic dermatitis and edema of the eyelid skin, allergic blepharitis, conjunctivitis, keratitis, iritis, iridocyclitis, retinitis, optic neuritis develop.
Allergic conjunctivitis is often combined with systemic diseases such as bronchial asthma, allergic rhinitis, and atopic dermatitis.
Hypersensitivity reactions (synonymous with allergies) are classified into immediate(develop within 30 minutes from the moment of exposure to the allergen) and slow(develop 24-48 hours later or later after exposure).
In some cases, the typical picture of the disease or its clear connection with the effects of an external allergenic factor leaves no doubt about the diagnosis. In pain
In most cases, the diagnosis of allergic eye diseases is associated with great difficulties and requires the use of specific allergological research methods.
Allergic history is the most important diagnostic factor. It should reflect data on hereditary allergic burden, features of the course of the disease, a set of effects that can cause an allergic reaction, the frequency and seasonality of exacerbations, the presence of allergic reactions, in addition to eye reactions. Naturally occurring or specially conducted elimination and exposure tests are of great diagnostic value. The first is to "turn off" the alleged allergen, the second - in the repeated exposure to them after the clinical phenomena subsided. Carefully collected anamnesis allows you to tentatively establish the "guilty" allergenic
agent.
Allergic skin tests are low-traumatic and at the same time quite reliable.
Provocative allergic tests (conjunctival, nasal and sublingual) are used only in exceptional cases and with great caution.
Laboratory allergy diagnostics is highly specific and is possible in the acute period of the disease without fear of causing harm to the patient.
The identification of eosinophils in scraping from the conjunctiva is of great diagnostic importance.
Basic principles of therapy:
Elimination, ie, exclusion, of the "culpable" allergen, if possible, is the most effective and safe method of preventing and treating allergic conjunctivitis;
Symptomatic drug therapy: local (with the use of ophthalmic drugs) and general (antihistamines by mouth for severe lesions) - takes the main place in the treatment of allergic conjunctivitis;
Specific immunotherapy is carried out in medical institutions with insufficient effectiveness of drug therapy and the impossibility of excluding the "guilty" allergen.
For antiallergic therapy, two groups of eye drops are used: the first - inhibiting the degranulation of mast cells: cromones - 2% lecroline solution, 2% lecroline solution without preservative, 2% cromohexal solution; the second - antihistamines: polynadym, spersallerg, opatanol, zaditen. Additionally, corticosteroid drugs are used: 0.1% dexamethasone solution (dexapos, maxidex, oftan-dexamethasone) and 1% or 2.5% hydrocortisone-POS solution, as well as non-steroidal anti-inflammatory drugs - 1% diclofenac solution (diclo-F, uniklofen) ...
The most common clinical forms of allergic conjunctivitis, characterized by treatment features: pollinous conjunctivitis, vernal keratoconjunctivitis, drug allergy, chronic allergic conjunctivitis, large papillary conjunctivitis.
Pollinous conjunctivitis.These are seasonal allergic eye diseases caused by pollen during the flowering period of grasses, cereals, and trees. The aggravation time is closely related to the pollination calendar of plants in each climatic region. Pollinous conjunctivitis can begin acutely: unbearable itching of the eyelids, burning under the eyelids, photophobia, lacrimation, edema and hypo-
Remia of the conjunctiva. Conjunctival edema can be so severe that the cornea "sinks" into the surrounding chemotic conjunctiva. In such cases, marginal infiltrates appear in the cornea, more often in the region of the palpebral fissure. Semi-transparent focal superficial infiltrates located along the limbus can merge and ulcerate, forming superficial corneal erosion. More often, pollinous conjunctivitis occurs chronically with moderate burning sensation under the eyelids, slight discharge, recurrent itching of the eyelids, mild conjunctival hyperemia, small follicles or papillae on the mucous membrane can be found.
Treatment for chronic course - zaditen or lecrolin 2 times a day for 2-3 weeks, for acute course - polynadym, opatanol or spersallerg 2-3 times a day. Additional therapy for severe cases: antihistamines by mouth for 10 days. For blepharitis, apply hydrocortisone ointment to the eyelids. In case of persistent recurrent course, specific immunotherapy is carried out under the supervision of an allergist.
Spring keratoconjunctivitis (spring catarrh). The disease usually occurs in children aged 3-7 years, has a predominantly chronic persistent, debilitating course. The clinical manifestations and prevalence of spring catarrh vary in different areas. The most characteristic clinical sign is papillary growths on the conjunctiva of the upper eyelid cartilage (conjunctival form), usually small, flattened, but can be large, deforming the eyelid (Fig. 9.6). Less commonly, papillary growths are located along the limbus (limbal form). Sometimes there is a mixed form. Often amazed

Rice. 9.6. Spring keratoconjunctivitis.
There is a cornea: epitheliopathy, erosion or corneal ulcer, keratitis, hyperkeratosis.
Treatment: with a mild course, instillation of zaditen or lecrolin is performed 3 times a day for 3-4 weeks. In severe cases, spersallerg or polynadym is used 2 times a day. In the treatment of spring catarrh, a combination of antiallergic drops with corticosteroids is necessary: instillation of eye drops (dexapos, maxidex or ophtan-dexamethasone) 2-3 times a day for 3-4 weeks. Additionally, antihistamines (diazolin, suprastin or claritin) are prescribed orally for 10 days. For corneal ulcers, reparative agents (eye drops taufon or gels solcoseryl, korneregel) are used 2 times a day until the condition of the cornea improves. With a long, persistent course of spring catarrh, a course of treatment with histoglobulin (4-10 injections) is carried out.
Medicinal allergic conjunctivitis. The disease can occur acutely after the first use of any medication, but usually develops chronically with prolonged treatment with the drug, and it is possible an allergic reaction as the primary drug,
and a preservative for eye drops. An acute reaction occurs within 1 hour after drug administration (acute drug conjunctivitis, anaphylactic shock, acute urticaria, Quincke's edema, systemic capillary toxicosis, etc.). A subacute reaction develops during the day (Fig. 9.7). A lingering reaction occurs over several days and weeks, usually with prolonged topical administration of drugs. Eye reactions of the latter type are the most common and chronic. Almost any drug can cause an allergic eye reaction. The same drug causes different manifestations in different patients. However, different drugs can cause a similar clinical picture of drug allergy.
The characteristic signs of acute allergic inflammation are hyperemia, edema of the eyelids and conjunctiva, lacrimation, and sometimes hemorrhage; chronic inflammation is characterized by itching of the eyelids, hyperemia of the mucous membrane, moderate discharge, and the formation of follicles. With drug allergy, the conjunctiva, cornea, eyelid skin are most often affected, much less often the choroid, retina, and optic nerve.

Rice. 9.7. Medicinal blepharoconjunctivitis.
The main thing in the treatment of drug allergy is to cancel the "guilty" drug or switch to the same drug without a preservative.
After the abolition of the "guilty" drug in the acute course, use eye drops polynadim, opatanol or spersallerg 2-3 times a day, in chronic - zaditen, cromohexal, lecrolin or lecrolin without preservative 2 times a day. With a severe and prolonged course, there may be a need to take antihistamines by mouth.
Chronic allergic conjunctivitis. Allergic conjunctivitis often occurs chronically: moderate burning of the eyes, slight discharge, recurrent itching of the eyelids. It should be borne in mind that often numerous complaints of discomfort are combined with minor clinical manifestations, which complicates the diagnosis.
Among the reasons for the persistent course may be increased sensitivity to pollen, industrial hazards, food products, household chemicals, house dust, dandruff and animal hair, dry fish food, medicines, cosmetics, contact lenses.
The most important treatment is to rule out risk factors for allergy development, if they can be identified. Local treatment includes instillation of lecroline or zaditen 2 times a day for 3-4 weeks. In case of blepharitis, hydrocortisone eye ointment is prescribed 2 times a day for the eyelids and instillation of artificial tears (natural tears, systein, oftagel) 2 times a day.
Allergic conjunctivitis when wearing contact lenses. It is believed that most contact lens wearers will eventually develop an
Lergic reaction of the conjunctiva: eye irritation, photophobia, lacrimation, burning under the eyelids, itching, discomfort when inserting the lens. On examination, you can find small follicles, small or large papillae on the conjunctiva of the upper eyelids, hyperemia of the mucous membrane, edema and pinpoint erosion of the cornea.
Treatment: it is necessary to stop wearing contact lenses. Prescribe instillations of lecrolin, cremohexal or zaditen 2 times a day. In case of an acute reaction, use polynadym or spersallerg 2 times a day.
Large papillary conjunctivitis (CPC). The disease is an inflammatory reaction of the conjunctiva of the upper eyelid, which has been in contact with a foreign body for a long period. The emergence of PDA is possible under the following conditions: wearing contact lenses (hard and soft), the use of eye prostheses, the presence of sutures after cataract extraction or keratoplasty, tightening scleral fillings.
Patients complain of itching and mucous discharge. In severe cases, ptosis may occur. Large (giant - with a diameter of 1 mm or more) papillae are grouped over the entire surface of the conjunctiva of the upper eyelids.
The clinical picture of CPC differs from the manifestations of the conjunctival form of spring catarrh in that all symptoms of CPC quickly disappear after the removal of the foreign body.
Until the symptoms disappear completely, zaditen or lecrolin is instilled 2 times a day. Wearing new contact lenses is possible only after the inflammatory phenomena have completely disappeared. For the prevention of PDA, systematic care of contact lenses and prostheses is required.
Prevention of allergic conjunctivitis. In order to prevent the disease, certain measures must be taken.
Elimination of causative factors (house dust, cockroaches, pets, dry fish food, household chemicals, cosmetics). It should be remembered that in patients with allergies, eye drops and ointments (especially antibiotics and antiviral agents) can cause not only allergic conjunctivitis, but also a general reaction in the form of urticaria and dermatitis.
If it is impossible to exclude contact with factors that cause allergies, lecrolin or cromohexal should be instilled as a preventive measure, one drop 1-2 times a day for 2 weeks prior to contact.
Upon contact with an allergen, opatanol, zaditen or spersallerg are instilled, which give an immediate effect that lasts for 12 hours.
With frequent relapses, specific immunotherapy is performed during the period of conjunctivitis remission.
9.2.3. Dystrophic diseases of the conjunctiva
This group of conjunctival lesions includes several diseases of various origins: keratoconjunctivitis dry, pinguecula, pterygoid hymen.
Dry eye syndrome (keratoconjunctivitis dry)- This damage to the conjunctiva and cornea, which occurs in connection with a pronounced decrease in the production of tear fluid and a violation of the stability of the tear film.
The tear film consists of three layers. Superficial, lipid,
the layer produced by the meibomian glands prevents the evaporation of fluid, thereby maintaining the stability of the lacrimal meniscus. The middle, aqueous, layer, which makes up 90% of the thickness of the tear film, is formed by the main and accessory lacrimal glands. The third layer, directly covering the corneal epithelium, is a thin mucin film produced by the goblet cells of the conjunctiva. Each layer of the tear film can be affected by various diseases, hormonal disorders, medicinal effects, which leads to the development of keratoconjunctivitis dry.
Dry eye syndrome is a widespread disease, especially in people over 70 years of age.
Patients complain of a feeling of a foreign body under the eyelids, burning, stinging, dryness in the eye, note photophobia, poor wind and smoke tolerance. All phenomena worsen in the evening. Eye irritation is caused by instillation of any eye drops. Objectively, dilated vessels of the scleral conjunctiva, a tendency to the formation of folds of the mucous membrane, flocculent inclusions in the lacrimal fluid, and the surface of the cornea dull. The following clinical forms of corneal lesions are distinguished, corresponding to the severity of the disease: epitheliopathy (barely noticeable or pinpoint defects of the corneal epithelium, detected by staining with fluorescein or rose Bengal), corneal erosion (more extensive epithelial defects), filamentous keratitis (epithelial flaps of filaments twisted in the form one end fixed to the cornea), corneal ulcer.
When diagnosing dry eye syndrome, the characteristic complaints of the patient are taken into account, the results of biomicro-
scopic examination of the edges of the eyelids, conjunctiva and cornea, as well as special tests.
1. Test according to Norn to assess the stability of the tear film. When looking down, with the upper eyelid pulled back, a 0.1-0.2% solution of fluorescein is instilled into the limbus area at 12 o'clock. After turning on the slit lamp, the patient should not blink. Observing the painted surface of the tear film, the time of the film rupture (black spot) is determined. The tear film rupture time of less than 10 s is of diagnostic value.
2. Schirmer's test with a standard strip of filter paper, one end inserted behind the lower eyelid. After 5 minutes, the strip is removed and the length of the wetted part is measured: its value less than 10 mm indicates a slight decrease in the production of tear fluid, and less than 5 mm - about a significant one.
3.A test with a 1% solution of Rose Bengal is especially informative, as it allows you to identify dead (stained) cells of the epithelium covering the cornea and conjunctiva.
Diagnosis of dry eye syndrome is associated with great difficulties and is based only on the results of a comprehensive assessment of the patient's complaints and clinical picture, as well as the results of functional tests.
Treatment remains challenging and involves gradual, individualized drug selection. Eye drops containing a preservative are less tolerated by patients and can cause an allergic reaction, so preference should be given to eye drops without a preservative. The main place is occupied by means of tear replacement therapy. Natural tears, systein, hyphens, chilo-chest of drawers are used 3-8 times a day, and the gel compositions of Oftagel or Vi-
disik-gel - 2-4 times a day. In case of allergic irritation of the conjunctiva, add zaditen, lecrolin or lecrolin without preservative (2 times a day for 2-3 weeks). In case of damage to the cornea, drops of vitasik, balarpan, hydromelose P, hilazar-chest of drawers, taufon or solcoseryl gel or korneregel are used.
Pinguecula(wen)- This
an irregularly shaped elastic formation slightly rising above the conjunctiva, located a few millimeters from the limbus within the palpebral fissure on the nasal or temporal side. Usually occurs in older people symmetrically in both eyes. Pinguecula does not cause painful sensations, although it attracts the patient's attention. No treatment is required, except in rare cases when the pinguecula becomes inflamed. In this case, anti-inflammatory eye drops (dexapos, maxidex, oftan-dexamethasone or hydrocortisone) are used, and when pinguecula is combined with a mild secondary bacterial infection, complex preparations (dexagentamicin or maxitrol) are used.
Pterygoid hymen (pterygium)- a flat superficial vascularized fold of the conjunctiva of a triangular shape, growing on the cornea. Irritating factors (wind, dust, temperature changes) can stimulate the growth of the pterygium, which leads to visual impairment. The pterygium slowly moves towards the center of the cornea, tightly connects with the Bowman's membrane and the superficial layers of the stroma. To delay the growth of pterygium and prevent relapse, anti-inflammatory and antiallergic agents are used (Zaditen drops, lecrolin, dexapos, maxidex, ophtan-dexamethasone, hydrocortisone or diclof). Surgical treatment needed
carry out during the period when the film has not yet covered the central part of the cornea. When the recurrent pterygium is excised, a marginal layer-by-layer keratoplasty is performed.
Questions for self-control
1. Function of the conjunctiva.
2. General clinical manifestations of acute conjunctivitis.
3. Basic principles of treatment of bacterial and allergic conjunctivitis.
4.What is the difference between the epidemic ke-
ratoconjunctivitis from adenoviral and hemorrhagic?
5. Clinical manifestations and treatment of trachoma. Complications and consequences.
6. Clinical manifestations and treatment of chlamydial conjunctivitis.
7.Prevention of gonococcal and chlamydial conjunctivitis of newborns.
8.What are pinguecula and pterygium?
9.Advantages and disadvantages of preservative-free eye drops. How does a tear film form on the surface of the conjunctiva and cornea? The meaning of the tear film.
The conjunctiva is the thin mucous membrane that lines the back of the eyelids and the anterior surface of the eyeball down to the cornea. The conjunctiva is a mucous membrane richly supplied with blood vessels and nerves. She easily responds to any irritation. The conjunctiva performs protective, moisturizing, trophic and barrier functions.
The conjunctiva forms a slit-like cavity (sac) between the eyelid and the eye, which contains the capillary layer of the tear fluid. Medially the conjunctival sac reaches the inner corner of the eye, where the lacrimal meatus and the semilunar fold of the conjunctiva (vestigial third eyelid) are located. Laterally the border of the conjunctival sac extends beyond the outer corner of the eyelids.
There are 3 parts of the conjunctiva:
- conjunctiva of the eyelids,
- conjunctiva of the fornix (upper and lower)
- conjunctiva of the eyeball.
The conjunctiva is a thin and delicate mucous membrane composed of
- superficial epithelial layer
- deep- submucosal layers. It contains lymphoid elements and various glands, including the lacrimal glands, which provide the production of mucin and lipids for the superficial tear film that covers the cornea. Krause's accessory lacrimal glands are located in the conjunctiva of the superior fornix. They are responsible for the constant production of tear fluid under normal, non-extreme conditions.
Glandular formations can become inflamed, which is accompanied by hyperplasia of lymphoid elements, an increase in glandular discharge and other phenomena (folliculosis, follicular conjunctivitis).
Eyelid conjunctiva
The conjunctiva of the eyelids is moist, pale pinkish in color, but sufficiently transparent, through it you can see the translucent glands of the eyelid cartilage (meibomian glands). The superficial layer of the eyelid conjunctiva is lined with a multi-row columnar epithelium, which contains a large number of goblet cells that produce mucus.
Under normal physiological conditions, this mucus is small. Goblet cells respond to inflammation by increasing the number and increasing secretion. When the conjunctiva of the eyelid is infected, the goblet cell discharge becomes mucopurulent or even purulent.
In the first years of life in children, the conjunctiva of the eyelids is smooth due to the absence of adenoid formations here. With age, the formation of focal accumulations of cellular elements in the form of follicles is observed, which determine the special forms of follicular lesions of the conjunctiva. An increase in glandular tissue predisposes to the appearance of folds, depressions and elevations that complicate the surface relief of the conjunctiva, closer to its arches, in the direction of the free edge of the eyelids, the folding is smoothed out.
Conjunctiva of the arches
In the vaults (fornix conjunctivae), where the conjunctiva of the eyelids passes into the conjunctiva of the eyeball, the epithelium changes from a multilayer cylindrical to a multilayer flat one.
Compared with other departments in the area of the fornices, the deep layer of the conjunctiva is more pronounced. Here, numerous glandular formations are well developed, up to small additional lacrimal glands (Krause's glands).
Under the transitional folds of the conjunctiva lies a pronounced layer of loose tissue. This circumstance determines the ability of the vault conjunctiva to fold and expand easily, which allows the eyeball to maintain full mobility. Cicatricial changes in the fornices of the conjunctiva limit the movement of the eye. Loose tissue under the conjunctiva contributes to the formation of edema here in inflammatory processes or stagnant vascular phenomena. The superior conjunctival fornix is more extensive than the inferior one. The depth of the first is 10-11 mm, and the second is 7-8 mm. Usually, the superior fornix of the conjunctiva extends beyond the superior orbitopalpebral sulcus, and the inferior fornix is at the level of the inferior orbitopalpebral fold. In the upper-outer part of the upper fornix, pinpoint holes are visible, these are the mouths of the excretory ducts of the lacrimal gland
Conjunctiva of the eyeball
It distinguishes between a movable part, covering the eyeball itself, and a part of the limbus region, soldered to the underlying tissue. From the limbus, the conjunctiva passes to the anterior surface of the cornea, forming its epithelial, optically completely transparent layer.
The genetic and morphological commonality of the epithelium of the conjunctiva of the sclera and cornea determines the possibility of the transition of pathological processes from one part to another. This occurs in trachoma even in its initial stages, which is essential for diagnosis.
In the conjunctiva of the eyeball, the adenoid apparatus of the deep layer is poorly represented, it is completely absent in the corneal region. The stratified squamous epithelium of the conjunctiva of the eyeball is non-keratinizing and retains this property under normal physiological conditions.
The conjunctiva of the eyeball is much more abundant than the conjunctiva of the eyelids and vaults, equipped with sensitive nerve endings (the first and second branches of the trigeminal nerve). In this regard, getting into the conjunctival sac of even small foreign bodies or chemicals causes a very unpleasant sensation. It is more significant in conjunctival inflammation.
The conjunctiva of the eyeball is not always connected with the underlying tissues in the same way. Along the periphery, especially in the upper outer part of the eye, the conjunctiva lies on a layer of loose tissue and here it can be freely moved with the instrument. This circumstance is used when performing plastic surgeries when it is required to move parts of the conjunctiva.
Along the perimeter of the limbus, the conjunctiva is fixed quite firmly, as a result of which, with significant edema, a vitreous shaft is formed in this place, sometimes hanging over the cornea with its edges.
The vascular system of the conjunctiva is part of the general circulatory system of the eyelids and eyes. The main vascular distributions are located in its deep layer and are represented mainly by the links of the microcircular network.
Many intramural blood vessels of the conjunctiva provide the vital activity of all its structural components. By changing the pattern of the vessels of certain areas of the conjunctiva (conjunctival, pericorneal and other types of vascular injections), differential diagnosis of diseases associated with the pathology of the eyeball itself, with diseases of purely conjunctival origin is possible.
Blood supply
The conjunctiva of the eyelids and eyeball is supplied from the arterial arches of the upper and lower eyelids and from the anterior ciliary arteries. Arterial arches of the eyelids are formed from the lacrimal and anterior ethmoid arteries. The anterior ciliary vessels are branches of the muscle arteries that supply blood to the outer muscles of the eyeball. Each muscular artery gives off two anterior ciliary arteries. An exception is the artery of the external rectus muscle, which gives off only one anterior ciliary artery.
The specified vessels of the conjunctiva, the source of which is the ophthalmic artery, belong to the system of the internal carotid artery. However, the lateral arteries of the eyelids, from which the branches supplying part of the conjunctiva of the eyeball originate, anastomose with the superficial temporal artery, which is a branch of the external carotid artery.
The blood supply to most of the conjunctiva of the eyeball is carried out by branches originating from the arterial arches of the upper and lower eyelids. These arterial branches and their accompanying veins form the conjunctival vessels, which in the form of numerous trunks go to the conjunctiva of the sclera from both anterior folds. The anterior ciliary arteries of the scleral tissue go over the area of attachment of the tendons of the rectus muscles towards the limbus. 3-4 mm from it, the anterior ciliary arteries are divided into superficial and perforating branches, which penetrate through the sclera into the eye, where they participate in the formation of the large arterial circle of the iris.
The superficial (recurrent) branches of the anterior ciliary arteries and their accompanying venous trunks are the anterior conjunctival vessels. The superficial branches of the conjunctival vessels and the posterior conjunctival vessels anastomosed with them form the superficial (subepithelial) ate of the vessels of the conjunctiva of the eyeball. In this layer, the elements of the microcircular bed of the bulbar conjunctiva are most abundant.
The branches of the anterior ciliary arteries, anastomosed with each other, as well as the tributaries of the anterior ciliary veins, form the circumference of the limbus, the marginal or perilimbal vasculature of the cornea.
Chicken breast cutlets
Coconut milk recipe
Kiwi ice cream, making sour sherbet
Clean fillet. Cutting fish. How to cut fish correctly
Delicious baked chicken in the oven with eggplant and tomatoes Recipe for eggplant with chicken breast in the oven