Cardiovascular disease is the most common cause of death in postindustrial societies. Timely diagnosis and therapy of the organs of the cardiovascular system helps to reduce the risk of developing heart pathologies among the population.
The electrocardiogram (ECG) is one of the simplest and most informative methods for studying cardiac activity. The ECG records the electrical activity of the heart muscle and displays the information in the form of prongs on paper tape.
ECG results are used in cardiology to diagnose various diseases. Heart alone is not recommended, it is better to consult a specialist. However, to get a general idea, it is worth knowing what the cardiogram shows.
Indications for ECG
In clinical practice, there are several indications for electrocardiography:
- severe chest pain;
- persistent fainting;
- dyspnea;
- intolerance to physical activity;
- dizziness;
- heart murmurs.
With a routine examination, an ECG is a mandatory diagnostic method. There may be other indications, which are determined by the attending physician. If you have any other alarming symptoms, see your doctor immediately to determine their cause.
How to decipher the cardiogram of the heart?
A strict plan for decoding the ECG consists of analyzing the resulting graph. In practice, only the total vector of the QRS complex is used. The work of the heart muscle is presented in the form of a continuous line with marks and alphanumeric designations. Anyone can decipher the ECG with a certain preparation, but only a doctor can make the correct diagnosis. ECG analysis requires knowledge of algebra, geometry and an understanding of lettering.
ECG indicators, which must be addressed when decoding the results:
- intervals;
- segments;
- teeth.
There are strict indicators of the norm on the ECG, and any deviation is already a sign of violations in the work of the heart muscle. Pathology can be excluded only by a qualified specialist - a cardiologist.
ECG decoding in adults - the norm in the table
ECG analysis
The ECG records cardiac activity in twelve leads: 6 limb leads (aVR, aVL, aVF, I, II, III) and six chest leads (V1-V6). The P wave reflects the process of excitation and relaxation of the atria. The Q, S waves show the phase of depolarization of the interventricular septum. R - wave denoting depolarization of the lower chambers of the heart, and T-wave - relaxation of the myocardium.
 Electrocardiogram analysis
Electrocardiogram analysis The QRS complex shows the time of ventricular depolarization. The time taken for the electrical pulse to travel from the SA node to the AV node is measured by the PR interval.
The computers built into most ECG devices are capable of measuring the time it takes for an electrical pulse to travel from the SA node to the ventricles. These measurements can help your doctor evaluate your heart rate and j, yfhe; bnm some types of heart block.
Computer programs can also interpret ECG results. And as artificial intelligence and programming have improved, they are often more accurate. However, the interpretation of the ECG has a lot of subtleties, so the human factor is still an important part of the assessment.
In the electrocardiogram, there may be deviations from the norm, which do not affect the patient's quality of life. However, there are standards for normal indicators of cardiac activity that are accepted by the international cardiological community.
Based on these standards, a normal electrocardiogram in a healthy person looks like this:
- rR interval - 0.6-1.2 seconds;
- P-wave - 80 milliseconds;
- PR interval - 120-200 milliseconds;
- pR segment - 50-120 milliseconds;
- qRS complex - 80-100 milliseconds;
- J-wave: absent;
- sT segment - 80-120 milliseconds;
- T-wave - 160 milliseconds;
- sT interval - 320 milliseconds;
- qT interval is 420 milliseconds or less if the heart rate is sixty beats per minute.
- ind. juice. - 17.3.
 Normal ECG
Normal ECG Pathological ECG parameters
The ECG in normal and in pathology is significantly different. Therefore, it is necessary to carefully approach the decoding of the cardiogram of the heart.
QRS complex
Any abnormality in the electrical system of the heart causes an elongation of the QRS complex. The ventricles have more muscle mass than the atria, so the QRS complex is significantly longer than the P wave. The duration, amplitude, and morphology of the QRS complex are useful in detecting cardiac arrhythmias, conduction abnormalities, ventricular hypertrophy, myocardial infarction, electrolyte abnormalities, and other painful conditions.
Q, R, T, P, U prongs
Abnormal Q-waves occur when an electrical signal travels through damaged heart muscle. They are considered markers of previous myocardial infarction.
R-wave depression is usually also associated with myocardial infarction, but it can also be caused by left bundle branch block, WPW syndrome, or hypertrophy of the lower chambers of the heart muscle.
 Table of ECG indicators is normal
Table of ECG indicators is normal T-wave inversion is always considered abnormal on the ECG tape. Such a wave can be a sign of coronary ischemia, Wellens syndrome, hypertrophy of the lower heart chambers, or a CNS disorder.
P wave with increased amplitude may indicate hypokalemia and hypertrophy of the right atrium. Conversely, a P wave with reduced amplitude may indicate hyperkalemia.
U-waves are most often observed in hypokalemia, but can also be present with hypercalcemia, thyrotoxicosis, or the use of epinephrine, class 1A and 3 antiarrhythmic drugs. They are often found in congenital long QT syndrome and intracranial hemorrhage.
An inverted U-wave may indicate pathological changes in the myocardium. Another U-wave can sometimes be seen on the ECG of athletes.
QT, ST, PR intervals
QTc prolongation induces premature action potentials during the late phases of depolarization. This increases the risk of developing ventricular arrhythmias or fatal ventricular fibrillation. Higher rates of QTc prolongation are observed in women, older patients, hypertensive patients and people of short stature.
The most common causes of a prolonged QT interval are hypertension and certain medications. The calculation of the interval duration is carried out according to the Bazett formula. With this sign, the decoding of the electrocardiogram should be performed taking into account the medical history. Such a measure is necessary to exclude hereditary influence.
ST interval depression may indicate coronary ischemia, transmural myocardial infarction, or hypokalemia.
 Characteristics of all indicators of electrocardiographic research
Characteristics of all indicators of electrocardiographic research An extended PR interval (greater than 200 ms) may indicate first-degree heart block. Elongation may be associated with hypokalemia, acute rheumatic fever, or Lyme disease. A short PR interval (less than 120 ms) may be associated with Wolff-Parkinson-White syndrome or Laun-Ganong-Levine syndrome. Depression in the PR segment may indicate atrial trauma or pericarditis.
Examples of heart rate description and ECG interpretation
Normal sinus rhythm
Sinus rhythm is any heart rhythm in which the excitation of the heart muscle starts from the sinus node. It is characterized by correctly oriented P waves on the ECG. By convention, the term "normal sinus rhythm" includes not only normal P waves, but all other ECG measurements.
 ECG norm and interpretation of all indicators
ECG norm and interpretation of all indicators ECG norm in adults:
- heart rate from 55 to 90 beats per minute;
- regular rhythm;
- normal interval of PR, QT and QRS complex;
- The QRS complex is positive in almost all leads (I, II, AVF and V3-V6) and negative in aVR.
Sinus bradycardia
The heart rate is less than 55 with sinus rhythm is called bradycardia. ECG decoding in adults should take into account all parameters: sports, smoking, medical history. Because in some cases, bradycardia is a variant of the norm, especially in athletes.
Pathological bradycardia occurs with weak sinus syndrome and is recorded on an ECG at any time of the day. This condition is accompanied by constant fainting, pallor and hyperhidrosis. In extreme cases, with malignant bradycardia, pacemakers are prescribed.
 Sinus bradycardia
Sinus bradycardia Signs of pathological bradycardia:
- heart rate less than 55 beats per minute;
- sinus rhythm;
- p waves are vertical, sequential and normal in morphology and duration;
- pR interval from 0.12 to 0.20 seconds;
Sinus tachycardia
The correct rhythm with a high heart rate (above 100 beats per minute) is commonly called sinus tachycardia. Note that normal heart rate varies with age, for example, infants may have a heart rate of 150 beats per minute, which is considered normal.
Advice! At home, with severe tachycardia, severe coughing or pressure on the eyeballs may help. These actions stimulate the vagus nerve, which activates the parasympathetic nervous system, causing the heart to beat more slowly.
 Sinus tachycardia
Sinus tachycardia Signs of pathological tachycardia:
- Heart rate above one hundred beats per minute;
- sinus rhythm;
- p waves are vertical, consistent and normal in morphology;
- the PR interval ranges between 0.12-0.20 seconds and decreases with an increase in heart rate;
- QRS complex less than 0.12 seconds.
Atrial fibrillation
Atrial fibrillation is an abnormal heart rhythm characterized by rapid and irregular atrial contraction. Most episodes are asymptomatic. Sometimes an attack is accompanied by the following symptoms: tachycardia, fainting, dizziness, shortness of breath, or chest pain. The disease is associated with an increased risk of heart failure, dementia, and stroke.
 Atrial fibrillation
Atrial fibrillation Signs of atrial fibrillation:
- Heart rate is constant or accelerated;
- p waves are absent;
- electrical activity is chaotic;
- RR intervals are irregular;
- QRS complex less than 0.12 seconds (in rare cases, the QRS complex lengthens).
Important! Despite the above explanations with the decoding of the data, only a qualified specialist - a cardiologist or general doctor - should make an ECG conclusion. Deciphering an electrocardiogram and differential diagnosis requires a higher medical education.
How to "read" myocardial infarction on an ECG?
Students who begin the study of cardiology often have the question of how to learn how to read a cardiogram correctly and identify myocardial infarction (MI)? There are several signs that you can “read” a heart attack on a paper tape:
- elevation of the ST segment;
- pointed T wave;
- deep Q wave or lack thereof.
In the analysis of the results of electrocardiography, these indicators are firstly identified, and then they are dealt with with others. Sometimes the earliest sign of acute myocardial infarction is only a pointed T wave. In practice, this is quite rare because it appears only 3-28 minutes after the onset of a heart attack.
Cardiology
Chapter 5. Analysis of the electrocardiogram


in. Conduction disturbances.Blockade of the anterior branch of the left bundle branch, blockade of the posterior branch of the left bundle branch, complete left bundle branch block, right bundle branch block, 2nd degree AV block and complete AV block.
g. Arrhythmias - see Ch. four.
Vi. Electrolyte disturbances
AND. Hypokalemia.PQ interval lengthening. Expansion of the QRS complex (rare). Pronounced U wave, flattened inverted T wave, depression of the ST segment, slight lengthening of the QT interval.
B. Hyperkalemia
Easy (5.5-6.5 meq / l). High pointed symmetrical T wave, shortening of the QT interval.
Moderate(6.5-8.0 meq / l). Decrease in the amplitude of the P wave; lengthening of the PQ interval. Expansion of the QRS complex, decrease in the amplitude of the R wave. Depression or elevation of the ST segment. Ventricular premature beats.
Heavy(9-11 meq / l). Absence of the P wave. Expansion of the QRS complex (up to sinusoidal complexes). Slow or accelerated idioventricular rhythm, ventricular tachycardia, ventricular fibrillation, asystole.
IN. Hypocalcemia.Prolongation of the QT interval (due to lengthening of the ST segment).
G. Hypercalcemia.Shortening of the QT interval (due to the shortening of the ST segment).
Vii. Action of medicines
AND. Cardiac glycosides
Therapeutic action.PQ interval lengthening. Oblique depression of the ST segment, shortening of the QT interval, changes in the T wave (flattened, inverted, biphasic), pronounced U wave. Decreased heart rate in atrial fibrillation.
Toxic effect. Ventricular premature beats, AV block, atrial tachycardia with AV block, accelerated AV nodal rhythm, sinoatrial block, ventricular tachycardia, bidirectional ventricular tachycardia, ventricular fibrillation.
AND. Dilated cardiomyopathy.Signs of enlargement of the left atrium, sometimes the right atrium. Low amplitude of the teeth, pseudoinfarction curve, blockade of the left bundle branch, anterior branch of the left bundle branch. Nonspecific changes in the ST segment and T wave. Ventricular premature beats, atrial fibrillation.
B. Hypertrophic cardiomyopathy.Signs of enlargement of the left atrium, sometimes the right atrium. Signs of left ventricular hypertrophy, abnormal Q waves, pseudoinfarction curve. Nonspecific ST segment and T wave changes In apical left ventricular hypertrophy, giant negative T waves in the left chest leads. Supraventricular and ventricular rhythm disturbances.
IN. Amyloidosis of the heart. Low amplitude of teeth, pseudo-infarction curve. Atrial fibrillation, AV blockade, ventricular arrhythmias, sinus node dysfunction.
G. Duchenne myopathy.Shortening the PQ interval. High R wave in leads V 1, V 2; deep Q wave in leads V 5, V 6. Sinus tachycardia, atrial and ventricular premature beats, supraventricular tachycardia.
D. Mitral stenosis.Signs of an enlarged left atrium. There is hypertrophy of the right ventricle, deviation of the electrical axis of the heart to the right. Often - atrial fibrillation.
E. Mitral valve prolapse. T-waves are flattened or negative, especially in lead III; depression of the ST segment, slight lengthening of the QT interval. Ventricular and atrial premature beats, supraventricular tachycardia, ventricular tachycardia, sometimes atrial fibrillation.
J. Pericarditis.Depression of the PQ segment, especially in leads II, aVF, V 2 —V 6. Diffuse rise of the ST segment with a bulge upward in leads I, II, aVF, V 3 —V 6. Sometimes - depression of the ST segment in lead aVR (in rare cases - in leads aVL, V 1, V 2). Sinus tachycardia, atrial rhythm disturbances. ECG changes go through 4 stages:
sT segment elevation, T wave normal;
the ST segment descends to the isoline, the T wave amplitude decreases;
the ST segment on the isoline, the T wave is inverted;
the ST segment on the isoline, the T wave is normal.
Z. Large pericardial effusion. Low amplitude of teeth, alternation of the QRS complex. The pathognomonic sign is complete electrical alternation (P, QRS, T).
AND. Dextrocardia.The P wave is negative in lead I. QRS complex inverted in lead I, R / S< 1 во всех грудных отведениях с уменьшением амплитуды комплекса QRS от V 1 к V 6 . Инвертированный зубец T в I отведении.
TO. Atrial septal defect.Signs of enlargement of the right atrium, less often the left atrium; lengthening of the PQ interval. RSR "in lead V 1; the electrical axis of the heart is deflected to the right with a defect of the ostium secundum type, to the left - with a defect of the ostium primum type. Inverted T wave in leads V 1, V 2. Sometimes atrial fibrillation.
L. Pulmonary artery stenosis.Signs of enlargement of the right atrium. Hypertrophy of the right ventricle with a high R wave in leads V 1, V 2; deviation of the electrical axis of the heart to the right. Inverted T wave in leads V 1, V 2.
M. Sick sinus syndrome. Sinus bradycardia, sinoatrial block, AV block, sinus node arrest, bradycardia-tachycardia syndrome, supraventricular tachycardia, atrial fibrillation / flutter, ventricular tachycardia.
IX. Other diseases
AND. COPD.Signs of enlargement of the right atrium. Deviation of the electrical axis of the heart to the right, displacement of the transition zone to the right, signs of right ventricular hypertrophy, low amplitude of the teeth; ECG type S I —S II —S III. T wave inversion in leads V 1, V 2. Sinus tachycardia, AV nodal rhythm, conduction disturbances, including AV block, slowing of intraventricular conduction, bundle branch block.
B. TELA. Syndrome S I —Q III —T III, signs of right ventricular overload, transient complete or incomplete blockade of the right bundle branch, displacement of the electrical axis of the heart to the right. T wave inversion in leads V 1, V 2; nonspecific changes in the ST segment and the T wave. Sinus tachycardia, sometimes atrial rhythm disturbances.
IN. Subarachnoid hemorrhage and other lesions of the central nervous system. Sometimes - pathological Q wave. High wide positive or deep negative T wave, elevation or depression of the ST segment, pronounced U wave, pronounced lengthening of the QT interval. Sinus bradycardia, sinus tachycardia, AV-nodal rhythm, ventricular premature beats, ventricular tachycardia.
G. HypothyroidismPQ interval lengthening. Low amplitude of the QRS complex. Flattened T wave. Sinus bradycardia.
D. Chronic renal failure. ST segment lengthening (due to hypocalcemia), high symmetrical T waves (due to hyperkalemia).
E. Hypothermia.PQ interval lengthening. A notch in the end part of the QRS complex (Osborne's tooth - see). Prolongation of the QT interval, inversion of the T wave. Sinus bradycardia, atrial fibrillation, AV nodal rhythm, ventricular tachycardia.
THE EX .The main types of pacemakers are described by a three-letter code: the first letter indicates which chamber of the heart is stimulated (A - Atrium - atrium, V - Ventricle - ventricle, D - Dual - both atrium and ventricle), the second letter - the activity of which camera is perceived (A, V or D), the third letter denotes the type of response to the perceived activity (I - Inhibition - blocking, T - Triggering - launch, D - Dual - both). So, in the VVI mode, both the stimulating and receiving electrodes are located in the ventricle, and when spontaneous ventricular activity occurs, its stimulation is blocked. In DDD mode, both the atrium and the ventricle have two electrodes (stimulating and sensing). Response type D means that when spontaneous activity of the atrium occurs, its stimulation will be blocked, and after a programmed time interval (AV-interval) a stimulus will be issued to the ventricle; when spontaneous ventricular activity occurs, on the contrary, ventricular pacing will be blocked, and atrial pacing will start after a programmed VA interval. Typical single chamber pacemaker modes are VVI and AAI. Typical two-chamber ECS modes are DVI and DDD. The fourth letter is R ( Rate-adaptive) means that the pacemaker is able to increase the pacing rate in response to changes in motor activity or exercise-dependent physiological parameters (eg, QT interval, temperature).
AND. General principles of ECG interpretation
Assess the nature of the rhythm (own rhythm with periodic activation of the stimulator or imposed).
Determine which chamber (s) are stimulated.
Determine which camera (s) activity is perceived by the stimulator.
Determine the programmed pacemaker intervals (VA, VV, AV intervals) from atrial (A) and ventricular (V) pacing artifacts.
Determine the paced mode. It must be remembered that ECG-signs of a single-chamber pacemaker do not exclude the possibility of having electrodes in two chambers: for example, stimulated ventricular contractions can be observed both with single-chamber pacemakers and with two-chamber pacemakers, in which ventricular stimulation follows at a certain interval after the P wave (DDD mode) ...
Eliminate intrusion and detection violations:
and. obstruction disorders: there are stimulation artifacts, which are not followed by depolarization complexes of the corresponding chamber;
b. detection abnormalities: there are pacing artifacts that should be blocked with normal detection of atrial or ventricular depolarization.
B. Separate ECS modes
AAI.If the intrinsic rate falls below the programmed pacemaker rate, constant interval AA atrial pacing is initiated. With spontaneous atrial depolarization (and its normal detection), the pacemaker time counter is reset. If, after the specified AA interval, spontaneous atrial depolarization is not repeated, atrial pacing is initiated.
VVI.With spontaneous ventricular depolarization (and its normal detection), the pacemaker time counter is reset. If, after a predetermined VV interval, spontaneous ventricular depolarization is not repeated, ventricular pacing is triggered; otherwise, the time counter is reset again and the entire cycle starts over. In adaptive VVIR-pacemakers, the rhythm frequency increases with an increase in the level of physical activity (up to the set upper limit of the heart rate).

DDD.If the intrinsic rate falls below the programmed pacemaker rate, atrial (A) and ventricular (V) pacing is initiated at specified intervals between pulses A and V (AV interval) and between V pulses and subsequent A pulses (VA interval). With spontaneous or forced ventricular depolarization (and normal detection thereof), the pacemaker time counter is reset and the VA countdown begins. If spontaneous depolarization of the atria occurs in this interval, then atrial pacing is blocked; otherwise, an atrial impulse is issued. In case of spontaneous or imposed atrial depolarization (and its normal detection), the pacemaker time counter is reset and the AV interval starts counting. If spontaneous depolarization of the ventricles occurs in this interval, then ventricular pacing is blocked; otherwise, a ventricular impulse is issued.
IN. Pacemaker dysfunction and arrhythmias
Violation of intrusion.The artifact of stimulation is not followed by a depolarization complex, although the myocardium is not in the refractory stage. Causes: displacement of the stimulating electrode, perforation of the heart, an increase in the stimulation threshold (with myocardial infarction, taking flecainide, hyperkalemia), damage to the electrode or violation of its insulation, impaired pulse generation (after defibrillation or due to depletion of the power source), as well as incorrectly set pacemaker parameters.

Violation of detection.The time counter of the pacemaker is not reset when an intrinsic or imposed depolarization of the corresponding chamber occurs, which leads to an irregular rhythm (the imposed rhythm is superimposed on the intrinsic one). Reasons: low amplitude of the perceived signal (especially with ventricular extrasystole), incorrectly set sensitivity of the pacemaker, as well as the reasons listed above (see). It is often sufficient to reprogram the sensitivity of the pacemaker.
Oversensitivity of the pacemaker.At the expected time (after the appropriate interval), no stimulation occurs. T waves (P waves, myopotentials) are misinterpreted as R waves and the pacemaker time counter is reset. If the T wave is erroneously detected, the VA interval starts from it. In this case, the sensitivity or refractory period of the detection must be reprogrammed. You can also set the VA count from the T wave.

Blocking by myopotentials.Myopotentials arising from hand movements can be misinterpreted as potentials from the myocardium and block stimulation. In this case, the intervals between the imposed complexes become different, and the rhythm becomes incorrect. Most often, such violations occur when using unipolar pacemakers.
Circular tachycardia.Imposed rhythm with the maximum frequency for a pacemaker. It is observed when retrograde atrial excitation after ventricular pacing is sensed by the atrial electrode and triggers ventricular pacing. This is typical for a two-chamber pacemaker with atrial excitation detection. In such cases, it may be sufficient to increase the refractory period of detection.

Tachycardia induced by atrial tachycardia.Imposed rhythm with the maximum frequency for a pacemaker. It is observed when atrial tachycardia (eg, atrial fibrillation) occurs in patients with a dual-chamber pacemaker. Frequent atrial depolarization is sensed by the pacemaker and triggers ventricular pacing. In such cases, they switch to the VVI mode and eliminate the arrhythmia.
Currently in clinical practice it is widely used electrocardiography method (ECG). The ECG reflects the processes of excitation in the heart muscle - the emergence and spread of excitement.
There are various ways of recording the electrical activity of the heart, which differ from each other in the location of the electrodes on the surface of the body.
The cells of the heart, coming into a state of excitement, become a source of current and cause a field to appear in the environment surrounding the heart.
In veterinary practice, different lead systems are used for electrocardiography: the imposition of metal electrodes on the skin in the chest, heart, limbs and tail.
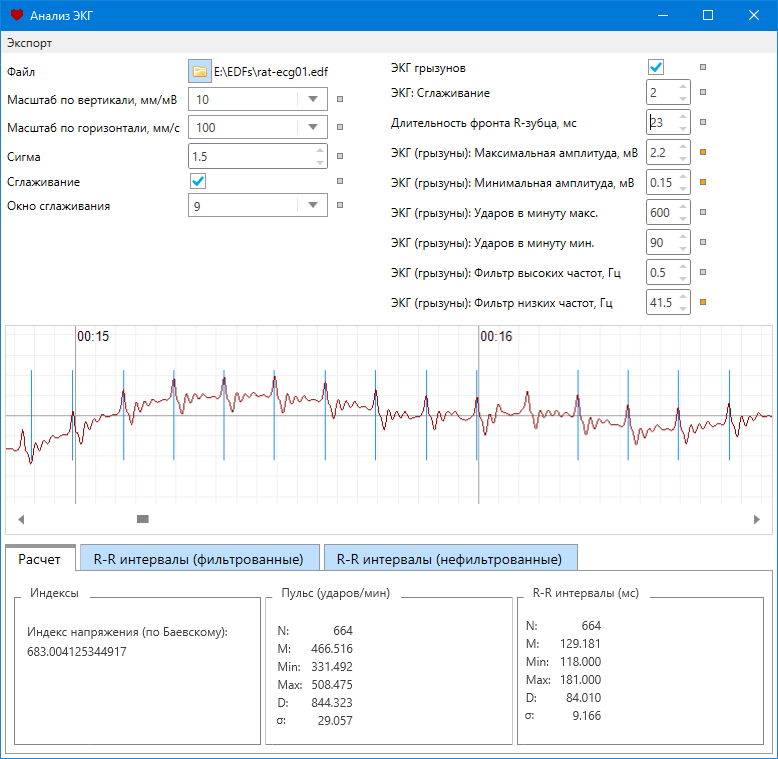
Electrocardiogram (ECG) - a periodically repeating curve of the biopotentials of the heart, reflecting the course of the process of excitation of the heart, which arose in the sinus (sinus-atrial) node and spreads throughout the heart, recorded using an electrocardiograph (Fig. 1).

Fig. 1. Electrocardiogram
Its individual elements - teeth and intervals - received special names: teeth R,Q, R, S, Tintervals R,PQ, QRS, QT, RR; segments PQ, ST, TP, characterizing the occurrence and spread of excitation through the atria (P), interventricular septum (Q), gradual excitation of the ventricles (R), maximum excitation of the ventricles (S), repolarization of the ventricles (S) of the heart. The P wave reflects the process of depolarization of both atria, a complex QRS- depolarization of both ventricles, and its duration is the total duration of this process. Segment ST and the G wave correspond to the phase of ventricular repolarization. Interval duration PQ is determined by the time it takes for excitation to pass through the atria. The duration of the QR-ST interval is the duration of the "electrical systole" of the heart; it may not correspond to the duration of the mechanical systole.
Low or medium heart rate and high voltage of ECG teeth are indicators of good fitness of the heart and high potential functional capabilities of lactation development in highly productive cows. A high heart rate with a high voltage of the ECG waves is a sign of a heavy load on the heart and a decrease in its potential. Reducing the voltage of the teeth R and T, increasing intervals P- Q and Q-T indicate a decrease in the excitability and conduction of the heart system and low functional activity of the heart.
ECG elements and principles of its general analysis
- a method of recording the potential difference of the electric dipole of the heart in certain parts of the human body. When the heart is excited, an electric field is generated that can be registered on the surface of the body.
Vectorcardiography - a method for studying the magnitude and direction of the integral electric vector of the heart during the cardiac cycle, the value of which is constantly changing.
Teleelectrocardiography (radioelectrocardiography electrotelecardiography) - a method of ECG registration, in which the recording device is significantly removed (from several meters to hundreds of thousands of kilometers) from the examined person. This method is based on the use of special sensors and transmitting and receiving radio equipment and is used when it is impossible or undesirable to carry out conventional electrocardiography, for example, in sports, aviation and space medicine.
Holter monitoring - 24-hour ECG monitoring with subsequent analysis of the rhythm and other electrocardiographic data. Daily ECG monitoring, along with a large volume of clinical data, makes it possible to reveal heart rate variability, which in turn is an important criterion for the functional state of the cardiovascular system.
Ballistocardiography - a method of recording micro-oscillations of the human body caused by the ejection of blood from the heart during systole and the movement of blood through large veins.
Dynamocardiography - a method of recording the displacement of the center of gravity of the chest, due to the movement of the heart and the movement of the mass of blood from the cavities of the heart into the vessels.
Echocardiography (ultrasound cardiography) - a method for examining the heart, based on the recording of ultrasonic vibrations reflected from the surfaces of the walls of the ventricles and atria at the border with the blood.
Auscultation - a method for assessing sound phenomena in the heart on the surface of the chest.
Phonocardiography - method of graphic registration of heart sounds from the surface of the chest.
Angiocardiography - an X-ray method for examining the cavities of the heart and great vessels after their catheterization and the introduction of radio-opaque substances into the blood. A variation of this method is coronary angiography -radiopaque examination of the vessels of the heart directly. This method is the "gold standard" in the diagnosis of coronary heart disease.
Rheography - a method for studying the blood supply to various organs and tissues, based on the registration of changes in the total electrical resistance of tissues when an electric current of high frequency and low strength passes through them.
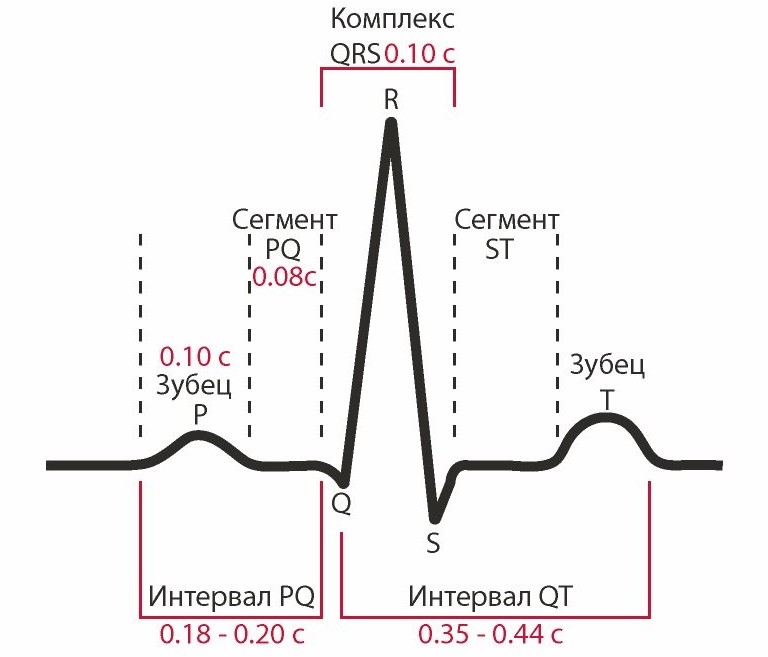
ECG is represented by teeth, segments and intervals (Fig. 2).

P wave under normal conditions characterizes the initial events of the cardiac cycle and is located on the ECG in front of the teeth of the ventricular complex QRS. It reflects the dynamics of excitation of the atrial myocardium. Barb R is symmetrical, has a flattened apex, its amplitude is maximum in lead II and is 0.15-0.25 mV, duration is 0.10 s. The ascending part of the tooth reflects depolarization mainly of the myocardium of the right atrium, the descending part of the left atrium. Normal tooth R positive in most leads, negative in lead aVR, in III and V1 leads, it can be biphasic. Changing the usual position of the prong Ron the ECG (in front of the complex QRS) observed with arrhythmias of the heart.
The processes of repolarization of the atrial myocardium are not visible on the ECG, since they are superimposed on the higher-amplitude teeth of the QRS complex.
IntervalPQ measured from the beginning of the prong R before the beginning of the wave Q... It reflects the time elapsed from the onset of atrial excitation to the onset of ventricular excitation or other in words, the time spent on conducting excitation along the conducting system to the ventricular myocardium. Its normal duration is 0.12-0.20 s and includes the time of the atrioventricular delay. Increasing the duration of the interval PQmore than 0.2 s may indicate a violation of the conduction of excitation in the area of \u200b\u200bthe atrioventricular node, bundle of His or its legs and is interpreted as evidence of a person having signs of a 1st degree conduction block. If an adult has an interval PQ less than 0.12 s, then this may indicate the existence of additional ways of conducting excitation between the atria and ventricles. Such people are at risk of developing arrhythmias.

Fig. 2. Normal values \u200b\u200bof ECG parameters in lead II
Teeth complex QRS reflects the time (normally 0.06-0.10 s) during which the structures of the ventricular myocardium are sequentially involved in the process of excitation. In this case, the papillary muscles and the outer surface of the interventricular septum are the first to be excited (a tooth Q duration up to 0.03 s), then the bulk of the ventricular myocardium (tooth duration 0.03-0.09 s) and last of all the base myocardium and the outer surface of the ventricles (tooth 5, duration up to 0.03 s). Since the mass of the left ventricular myocardium is significantly greater than the mass of the right, changes in electrical activity, namely in the left ventricle, dominate in the ventricular complex of the ECG teeth. Since the complex QRS reflects the process of depolarization of the powerful mass of the ventricular myocardium, then the amplitude of the teeth QRSusually higher than the amplitude of the wave R, reflecting the process of depolarization of a relatively small mass of the atrial myocardium. Wave amplitude R fluctuates in different leads and can reach up to 2 mV in I, II, III and in aVF leads; 1.1 mV in aVLand up to 2.6 mV in the left chest leads. Barbs Qand Sin some leads may not appear (Table 1).
Table 1. The boundaries of the normal values \u200b\u200bof the amplitude of the ECG waves in the II standard lead
|
ECG teeth |
Minimum rate, mV |
Maximum norm, mV |
SegmentSTis registered after the complex ORS. It is measured from the end of the prong Sbefore the beginning of the wave T.At this time, the entire myocardium of the right and left ventricles is in a state of excitation and the potential difference between them practically disappears. Therefore, the ECG recording becomes almost horizontal and isoelectric (normal segment deviation is allowed STfrom the isoelectric line by no more than 1 mm). Bias STa large value can be observed with myocardial hypertrophy, with severe physical exertion and indicates insufficient blood flow in the ventricles. Significant deviation STfrom the isoline, recorded in several ECG leads, can be a harbinger or evidence of the presence of myocardial infarction. Duration STin practice, it is not evaluated, since it significantly depends on the frequency of heart contractions.
T wavereflects the process of repolarization of the ventricles (duration - 0.12-0.16 s). The amplitude of the T wave is very variable and should not exceed 1/2 of the amplitude of the wave R. The G wave is positive in those leads in which a wave of significant amplitude is recorded R. In leads in which the tooth Rlow amplitude or not detected, a negative wave can be recorded T (leads AVRand VI).
IntervalQTreflects the duration of the "electrical systole of the ventricles" (the time from the beginning of their depolarization to the end of repolarization). This interval is measured from the beginning of the wave Qto the end of the prong T.Normally, at rest, it has a duration of 0.30-0.40 s. Interval duration FROM depends on the heart rate, the tone of the centers of the autonomic nervous system, hormonal levels, the action of certain medicinal substances. Therefore, the change in the duration of this interval is monitored in order to prevent overdose of certain cardiac medications.
BarbU is not a permanent element of the ECG. It reflects trace electrical processes observed in the myocardium of some people. No diagnostic value was received.
ECG analysis is based on assessing the presence of teeth, their sequence, direction, shape, amplitude, measuring the duration of the teeth and intervals, position relative to the isoline and calculating other indicators. Based on the results of this assessment, a conclusion is made about the heart rate, the source and correctness of the rhythm, the presence or absence of signs of myocardial ischemia, the presence or absence of signs of myocardial hypertrophy, the direction of the electrical axis of the heart and other indicators of heart function.
For the correct measurement and interpretation of ECG indicators, it is important that it was recorded with high quality under standard conditions. Such an ECG recording is of high quality, on which there are no noise and a shift of the recording level from the horizontal and the requirements of standardization are met. The electrocardiograph is an amplifier of biopotentials, and to set a standard gain on it, its level is selected when applying a calibration signal of 1 mV to the input of the device leads to a deviation of the record from the zero or isoelectric line by 10 mm. Compliance with the amplification standard allows you to compare ECGs recorded on any type of device and express the amplitude of the ECG waves in millimeters or millivolts. To correctly measure the duration of the waves and ECG intervals, the recording should be made at the standard speed of movement of the chart paper, writing device or the speed of the scan on the monitor screen. Most modern electrocardiographs will provide the ability to record ECG at three standard speeds: 25, 50 and 100 mm / s.
Having checked visually the quality and compliance with the standardization requirements of the ECG recording, they begin to assess its indicators.
The amplitude of the teeth is measured by taking the isoelectric, or zero, line as the reference point. The first is recorded in the case of the same potential difference between the electrodes (PQ - from the end of the P wave to the beginning of Q, the second - in the absence of a potential difference between the lead electrodes (TP interval)). The teeth directed upwards from the isoelectric line are called positive, downward ones - negative. A segment is a section of an ECG between two teeth, an interval is a section that includes a segment and one or more adjacent teeth.
The electrocardiogram can be used to judge the place of origin of excitation in the heart, the sequence of coverage of the heart with excitement, the speed of the excitation. Consequently, one can judge the excitability and conduction of the heart, but not the contractility. In some heart conditions, there may be a disconnection between the excitement and contraction of the heart muscle. In this case, the pumping function of the heart may be absent in the presence of registered biopotentials of the myocardium.
RR interval
The duration of the cardiac cycle is determined by the interval RR, which corresponds to the distance between the vertices of adjacent teeth R. The proper value (norm) of the interval QTcalculated by the Bazett formula:
![]()
where K -coefficient equal to 0.37 for men and 0.40 for women; RR - the duration of the cardiac cycle.
Knowing the duration of the heart cycle, it is easy to calculate the heart rate. To do this, it is enough to divide the time interval 60 s by the average length of the intervals RR.
Comparing the duration of a series of intervals RRit is possible to draw a conclusion about the correctness of the rhythm or the presence of arrhythmia in the work of the heart.
Comprehensive analysis of standard ECG leads can also detect signs of insufficient blood flow, metabolic disorders in the heart muscle and diagnose a number of heart diseases.
Heart tones- sounds that occur during systole and diastole are a sign of the presence of heart contractions. The sounds generated by the beating heart can be examined by auscultation and recorded by phonocardiography.
Auscultation (listening) can be carried out directly with the ear attached to the chest, and with the help of instruments (stethoscope, phonendoscope) that amplify or filter the sound. On auscultation, two tones are clearly audible: I tone (systolic), arising at the beginning of ventricular systole, II tone (diastolic), arising at the beginning of ventricular diastole. The first tone during auscultation is perceived as lower and longer (represented by frequencies of 30-80 Hz), the second - higher and shorter (represented by frequencies of 150-200 Hz).
The formation of the I tone is due to sound vibrations caused by the slamming of the AV valve leaflets, the trembling of the tendon filaments associated with them when they are pulled, and the contraction of the ventricular myocardium. Some contribution to the origin of the last part of the I tone can be made by the opening of the semilunar valves. The I tone is most clearly heard in the apical impulse of the heart (usually in the 5th intercostal space on the left, 1-1.5 cm to the left of the midclavicular line). Listening to its sound at this point is especially informative for assessing the state of the mitral valve. To assess the state of the tricuspid valve (overlapping the right AV opening), listening to 1 tone at the base of the xiphoid process is more informative.
The second tone is better heard in the 2nd intercostal space to the left and right of the sternum. The first part of this tone is due to the collapse of the aortic valve, the second - the pulmonary valve. On the left, the sound of the pulmonary valve is better heard, and on the right, the sound of the aortic valve.
With the pathology of the valve apparatus during the work of the heart, aperiodic sound vibrations occur, which create noise. Depending on which valve is damaged, they are superimposed on a specific heart sound.
A more detailed analysis of sound phenomena in the heart is possible with a recorded phonocardiogram (Fig. 3). To register a phonocardiogram, an electrocardiograph is used, complete with a microphone and an amplifier of sound vibrations (phonocardiographic attachment). The microphone is placed at the same points on the body surface where the auscultation is performed. For a more reliable analysis of heart sounds and murmurs, the phonocardiogram is always recorded simultaneously with the electrocardiogram.

Fig. 3. Synchronously recorded ECG (top) and phonocardnogram (bottom).
On the phonocardiogram, in addition to I and II tones, III and IV tones can be recorded, which are usually not audible by the ear. The third tone appears as a result of vibrations of the walls of the ventricles during their rapid filling with blood during the eponymous phase of diastole. The fourth tone is recorded during atrial systole (presystole). The diagnostic significance of these tones has not been determined.
The appearance of the I tone in a healthy person is always recorded at the beginning of the ventricular systole (period of tension, the end of the phase of asynchronous contraction), and its complete registration coincides in time with the recording on the ECG of the teeth of the ventricular complex QRS. The initial low-frequency oscillations of the I tone, small in amplitude (Fig. 1.8, a), are sounds arising from the contraction of the ventricular myocardium. They are recorded almost simultaneously with the Q wave on the ECG. The main part of the I tone, or the main segment (Fig. 1.8, b), is represented by high-frequency sound vibrations of large amplitude that occur when the AV valves are closed. The beginning of the registration of the main part of the I tone is delayed in time by 0.04-0.06 from the beginning of the wave Q on ECG (Q- I tone in fig. 1.8). The end part of the I tone (Fig. 1.8, c) is a small amplitude sound oscillations that occur when the valves of the aorta and pulmonary artery are opened and sound oscillations of the walls of the aorta and pulmonary artery. The duration of the first tone is 0.07-0.13 s.
The onset of the II tone in normal conditions coincides in time with the onset of ventricular diastole, delaying by 0.02-0.04 s to the end of the G wave on the ECG. The tone is represented by two groups of sound oscillations: the first (Fig. 1.8, a) is caused by the closure of the aortic valve, the second (P in Fig. 3) - by the closure of the pulmonary valve. The duration of the second tone is 0.06-0.10 s.
If by the elements of the ECG one can judge the dynamics of electrical processes in the myocardium, then by the elements of the phonocardiogram - about the mechanical phenomena in the heart. The phonocardiogram provides information about the state of the heart valves, the beginning of the isometric contraction and relaxation of the ventricles. The distance between I and II tone determines the duration of the "mechanical systole" of the ventricles. An increase in the amplitude of the II tone may indicate an increased pressure in the aorta or pulmonary trunk. However, at present, more detailed information about the state of the valves, the dynamics of their opening and closing and other mechanical phenomena in the heart is obtained by ultrasound examination of the heart.
Heart ultrasound
Ultrasound examination (ultrasound) of the heart, or echocardiography, is an invasive method for studying the dynamics of changes in the linear dimensions of the morphological structures of the heart and blood vessels, which makes it possible to calculate the rate of these changes, as well as changes in the volumes of the cavities of the heart and blood during the implementation of the cardiac cycle.
The method is based on the physical property of high-frequency sounds in the 2-15 MHz range (ultrasound) to pass through liquid media, tissues of the body and heart, while reflecting from the boundaries of any changes in their density or from the boundaries of organs and tissues.
A modern ultrasound (US) echocardiograph includes such units as an ultrasound generator, an ultrasound emitter, a receiver of reflected ultrasound waves, visualization and computer analysis. The emitter and the ultrasonic receiver are structurally combined in a single device called the ultrasonic sensor.
Echocardiographic examination is carried out by sending short series of ultrasound waves generated by the device from the sensor into the body in certain directions. Part of the ultrasound waves, passing through the tissues of the body, are absorbed by them, and the reflected waves (for example, from the interfaces between the myocardium and blood; valves and blood; walls of blood vessels and blood), propagate in the opposite direction to the body surface, are captured by the sensor receiver and are converted into electrical signals. After computer analysis of these signals, an ultrasound image of the dynamics of mechanical processes occurring in the heart during the cardiac cycle is formed on the display screen.
Based on the results of calculating the distances between the working surface of the sensor and the surfaces of sections of various tissues or changes in their density, it is possible to obtain a variety of visual and digital echocardiographic indicators of the heart. Among these indicators are the dynamics of changes in the size of the cavities of the heart, the size of the walls and partitions, the position of the valve cusps, the size of the inner diameter of the aorta and large vessels; identification of the presence of seals in the tissues of the heart and blood vessels; calculation of end-diastolic, end-systolic, stroke volumes, ejection fraction, rate of blood expulsion and filling of the heart cavities with blood, etc. Ultrasound of the heart and blood vessels is currently one of the most common, objective methods for assessing the state of morphological properties and pumping function of the heart.
Pathology of the cardiovascular system is one of the most common problems affecting people of all ages. Timely treatment and diagnostics of the circulatory system can significantly reduce the risk of developing dangerous diseases.
To date, the most effective and easily accessible method for examining the work of the heart is an electrocardiogram.
When examining the results of the patient's examination, doctors pay attention to such components of the ECG as:
- Teeth;
- Intervals;
- Segments.
Not only their presence or absence is assessed, but also the height, duration, location, direction and sequence.
There are strict norm parameters for each line on the ECG tape, the slightest deviation from which may indicate violationsin the work of the heart.
ECG analysis
The entire set of ECG lines is examined and measured mathematically, after which the doctor can determine some parameters of the heart muscle and its conducting system: heart rate, heart rate, pacemaker, conductivity, electrical axis of the heart.
To date, all these indicators are investigated by high-precision electrocardiographs.
Sinus heart rate
This is a parameter that reflects the rhythm of the heart contractions arising under the influence of the sinus node (normal). It shows the coherence of the work of all parts of the heart, the sequence of the processes of tension and relaxation of the heart muscle.
The rhythm is very easily identified by the tallest R-waves: if the distance between them is the same throughout the entire recording or deviates by no more than 10%, then the patient does not suffer from arrhythmia.
Heart rate
The number of beats per minute can be determined not only by counting the pulse, but also by the ECG. To do this, you need to know the speed with which the ECG was recorded (usually 25, 50 or 100 mm / s), as well as the distance between the highest teeth (from one vertex to the other).
Multiplying the recording time of one mm by segment length R-R, you can get the heart rate. Normally, its indicators range from 60 to 80 beats per minute.

Excitation source
The autonomic nervous system of the heart is designed in such a way that the contraction process depends on the accumulation of nerve cells in one of the zones of the heart. Normally, this is a sinus node, impulses from which diverge throughout the nervous system of the heart.
In some cases, the role of a pacemaker can be assumed by other nodes (atrial, ventricular, atrioventricular). You can determine this by examining the P wave is inconspicuous, located just above the isoline.
You can read detailed and comprehensive information about the symptoms of cardiosclerosis of the heart.
Conductivity
This is a criterion showing the process of impulse transmission. Normally, impulses are transmitted sequentially from one pacemaker to another, without changing the order.
Electric axle
An indicator based on the process of ventricular excitation. Mathematical analysis of Q, R, S waves in I and III leadsallows you to calculate a certain resulting vector of their excitation. This is necessary to establish the functioning of the branches of the His bundle.
The resulting angle of inclination of the heart axis is estimated by the value: 50-70 ° norm, 70-90 ° deviation to the right, 50-0 ° deviation to the left.
In cases where an inclination of more than 90 ° or more than -30 ° is observed, there is a serious disturbance in the work of the His bundle.
Prongs, segments and intervals
Prongs - ECG areas lying above the isoline, their meaning is as follows:
- P - reflects the processes of contraction and relaxation of the atria.
- Q, S- reflect the processes of excitation of the interventricular septum.
- R - the process of excitation of the ventricles.
- T - the process of relaxation of the ventricles.
Intervals - ECG areas lying on the isoline.
- PQ- reflects the propagation time of the impulse from the atria to the ventricles.
Segments are ECG sections that include an interval and a wave.
- QRST- the duration of the contraction of the ventricles.
- ST- the time of complete excitation of the ventricles.
- TP- time of electrical diastole of the heart.

The norm in men and women
Decoding of the ECG of the heart and the norm of indicators in adults are presented in this table:

Healthy baby results
Interpretation of the results of ECG measurements in children and their norm in this table:

Dangerous diagnoses
What dangerous conditions can be determined by ECG readings during decoding?
Extrasystole
This phenomenon characterized by a failure of the heart rate... The person feels a temporary increase in the frequency of contractions, followed by a pause. It is associated with the activation of other pacemakers, sending an additional burst of impulses along with the sinus node, which leads to an extraordinary contraction.
If extrasystoles appear no more than 5 times per hour, then they cannot cause significant harm to health.
Arrhythmia
Characterized changes in the frequency of sinus rhythmwhen the pulses arrive at different frequencies. Only 30% of these arrhythmias require treatment. able to provoke more serious diseases.
In other cases, this can be a manifestation of physical activity, a change in hormonal levels, the result of a fever and does not threaten health.

Bradycardia
It occurs when the sinus node is weakened, unable to generate impulses with the proper frequency, as a result of which the heart rate also slows down, up to 30-45 beats per minute.
Tachycardia
The opposite phenomenon, characterized by an increase in heart rate more than 90 beats per minute. In some cases, temporary tachycardia occurs under the influence of strong physical exertion and emotional stress, as well as during the period of illness associated with an increase in temperature.

Conduction disturbance
In addition to the sinus node, there are other underlying second- and third-order pacemakers. Normally, they conduct impulses from a first-order pacemaker. But if their functions are weakened, a person can feel weakness, dizzinesscaused by oppression of the heart.
It is also possible to lower blood pressure, because the ventricles will contract less frequently or irregularly.
Many factors can lead to disruptions in the work of the heart muscle itself. Tumors develop, muscle nutrition is disrupted, and depolarization processes fail. Most of these pathologies require serious treatment.
Why there may be differences in performance
In some cases, when re-analyzing the ECG, deviations from previously obtained results are revealed. With what it can be connected?
- Different time of day... Usually, an ECG is recommended to be done in the morning or afternoon, when the body has not yet had time to be exposed to stress factors.
- Loads... It is very important that the patient is calm when recording an ECG. The release of hormones can increase heart rate and distort readings. In addition, it is also not recommended to engage in heavy physical labor before the examination.
- Eating... Digestion affects circulation, and alcohol, tobacco and caffeine can affect heart rate and blood pressure.
- Electrodes... Incorrect overlap or accidental displacement can seriously change the indicators. Therefore, it is important not to move during the recording and to degrease the skin in the area where the electrodes are applied (the use of creams and other skin products before the examination is highly undesirable).
- Background... Sometimes other devices can interfere with the operation of the electrocardiograph.

Additional examination techniques
Halter
Method long-term study of the work of the heart, possible thanks to a portable compact tape recorder that is capable of recording results on magnetic tape. The method is especially good when it is necessary to investigate recurrent pathologies, their frequency and time of occurrence.

Treadmill
Unlike a conventional ECG recorded at rest, this method is based on an analysis of the results after exercise... Most often, this is used to assess the risk of possible pathologies that were not detected on a standard ECG, as well as when prescribing a course of rehabilitation for patients who have had a heart attack.
Phonocardiography
 Allows analyze heart sounds and murmurs. Their duration, frequency and time of occurrence correlate with the phases of cardiac activity, which makes it possible to assess the work of the valves, the risks of developing endo- and rheumatic heart disease.
Allows analyze heart sounds and murmurs. Their duration, frequency and time of occurrence correlate with the phases of cardiac activity, which makes it possible to assess the work of the valves, the risks of developing endo- and rheumatic heart disease.
A standard ECG is a graphical representation of all parts of the heart. Many factors can affect its accuracy, therefore you should follow the doctor's recommendations.
The examination reveals most of the pathologies of the cardiovascular system, however, additional tests may be required for an accurate diagnosis.
Finally, we suggest watching a video course on decoding "EKG can be done by everyone":
The electrocardiograph, using a sensor, registers and records the parameters of the heart's activity, which are printed on special paper. They look like vertical lines (teeth), the height and location of which relative to the axis of the heart are taken into account when decoding the picture. If the ECG is normal, the impulses are clear, straight lines that follow at a certain interval in a strict sequence.
The ECG study consists of the following indicators:
- Prong R. Responsible for the contraction of the left and right atria.
- P-Q interval (R) is the distance between the R wave and the QRS complex (the beginning of the Q wave or R wave). Shows the duration of the passage of the pulse through the ventricles, bundle of His and AV node back to the ventricles.
- The QRST complex is equal to the systole (the moment of muscle contraction) of the ventricles. The excitation wave propagates at different intervals in different directions, forming the Q, R, S waves.
- Q wave. Shows the beginning of the propagation of the impulse along the interventricular septum.
- S wave Reflects the end of the distribution of excitation through the interventricular septum.
- Prong R. Corresponds to the distribution of impulses to the right and left myocardium of the ventricles.
- Segment (R) ST. This is the path of the impulse from the end point of the S wave (in its absence, the R wave) to the beginning of the T.
- T wave Shows the process of repolarization of the ventricular myocardium (elevation of the gastric complex in the ST segment).
The video examines the main elements that make up an electrocardiogram. Taken from the MEDFORS channel.
How to decipher a cardiogram
- Age and gender.
- Cells on paper are composed of horizontal and vertical lines with large and small cells. Horizontal - are responsible for the frequency (time), vertical - this is voltage. A large square is equal to 25 small squares, each side of which is 1 mm and 0.04 seconds. The large square corresponds to the value of 5 mm and 0.2 seconds, and 1 cm of the vertical line is 1 mV of voltage.
- The anatomical axis of the heart can be determined using the vector of the direction of the teeth Q, R, S. Normally, the impulse should be conducted through the ventricles to the left and down at an angle of 30-70º.
- The reading of the teeth depends on the distribution vector of the excitation wave on the axis. The amplitude differs in different leads, and part of the pattern may be missing. The upward direction from the isoline is considered positive, downward - negative.
- The electrical axes of the leads Ι, ΙΙ, ΙΙΙ have a different location in relation to the axis of the heart, being displayed, respectively, with different amplitudes. Leads AVR, AVF and AVL show the difference in potentials between the limbs (with a positive electrode) and the average potential of the other two (with a negative one). The AVR axis is directed from bottom to top and to the right, so most of the teeth have negative amplitude. The AVL lead is perpendicular to the electrical axis of the heart (EOS), so the total QRS complex is close to zero.
Noise and sawtooth vibrations (up to 50 Hz) displayed in the picture may indicate the following:
- muscle tremor (small fluctuations with different amplitudes);
- chills;
- poor contact between the skin and the electrode;
- malfunction of one or more wires;
- interference from household electrical appliances.
Cardiac impulses are recorded using electrodes that connect the electrocardiograph to the human limbs and chest.
The paths along which the discharges (leads) follow are designated as follows:
- AVL (analogue of the first);
- AVF (analogue of the third);
- AVR (mirrored lead mapping).
Chest Lead Designations:
Prongs, segments and intervals
You can independently interpret the value of the indicators using the ECG norms for each of them:
- Wave P. Must have a positive value in leads Ι-and be biphasic in V1.
- PQ interval. It is equal to the sum of the time of contraction of the cardiac atria and their conduction through the AV node.
- Q wave. Must come before R and have a negative value. In compartments Ι, AVL, V5 and V6, it can be present up to a length of no more than 2 mm. Its presence in lead ΙΙΙ should be temporary and disappear after a deep breath.
- QRS complex. It is calculated by the cells: the normal width is 2-2.5 cells, the interval is 5, the amplitude in the thoracic region is 10 small squares.
- Segment S-T. To determine the value, you need to count the number of cells from point J. Normally, they are 1.5 (60 ms).
- T wave. Must match the QRS direction. Has a negative value in leads: ΙΙΙ, AVL, V1 and standard positive - Ι, ΙΙ, V3-V6.
- U-wave. If this indicator is displayed on paper, it can occur in close proximity to the T wave and merge with it. Its height is 10% of T in branches V2-V3 and indicates the presence of bradycardia.
How to calculate your heart rate
The heart rate calculation scheme looks like this:
- Identify high R waves on the ECG image.
- Find the large squares between the vertices R is the heart rate.
- Calculate using the formula: HR \u003d 300 / number of squares.
For example, there are 5 squares between the vertices. Heart rate \u003d 300/5 \u003d 60 beats / min.
Photo gallery
Research symbols The figure shows the normal sinus rhythm of the heart Atrial fibrillation Method for determining heart rate In the photo, the diagnosis of coronary heart disease Myocardial infarction on an electrocardiogram
What is an abnormal ECG
An abnormal electrocardiogram is an abnormality of the test results. The doctor's job in this case is to determine the level of danger of anomalies in the deciphering of the study.
Abnormal ECG results may indicate the following problems:
- the shape and size of the heart or one of its walls are markedly changed;
- imbalance of electrolytes (calcium, potassium, magnesium);
- ischemia;
- heart attack;
- change in the normal rhythm;
- side effect of the medications you are taking.
What does an ECG look like in normal and pathological conditions
The parameters of the electrocardiogram in adult men and women are presented in the table and look like this:
| ECG parameters | Norm | Deviation | Probable reason for rejection |
| R-R-R distance | Uniform spacing between teeth | Uneven distance |
|
| Heart rate | 60-90 bpm at rest | Below 60 or above 90 bpm at rest |
|
| Atrial contraction - R wave | Pointed upward, outwardly resembles an arc. The height is about 2mm. May not be present in ΙΙΙ, AVL, V1. |
|
|
| P-Q interval | Straight line between P-Q waves with an interval of 0.1-0.2 seconds. |
|
|
| QRS complex | Length 0.1 second - 5 mm, then a T wave and a straight line. |
|
|
| Q wave | Missing or pointing downward with a depth of 1/4 R-wave | Depth and / or width exceeding the norm |
|
| R wave | Height 10-15 mm, pointed upward. Present in all leads. |
|
|
| S wave | Depth 2-5 mm, the sharp end is directed downward. |
| Left ventricular hypertrophy. |
| Segment S-T | Matches the distance between the S-T waves. | Any deviation of the horizontal line by more than 2 mm. |
|
| T wave | The height of the arc is up to 1/2 of the R wave or the same (in the V1 segment). Direction is up. |
|
|
What should be a cardiogram in a healthy person
Readings for a good adult cardiogram:
The video presents a comparison of the cardiogram of a healthy and a sick person and gives the correct interpretation of the data obtained. Taken from the "Life of Hypertensive" channel.
Indicators in adults
An example of a normal ECG in adults:
Indicators in children
Electrocardiogram parameters in children:
Rhythm disturbances when decoding an ECG
Heart rhythm disturbances can be observed in healthy people and is a variant of the norm. The most common types of arrhythmias and deviations of the conducting system. In the process of interpreting the data obtained, it is important to take into account all the indicators of the electrocardiogram, and not each separately.
Arrhythmias
A heart rhythm disorder can be as follows:
- Sinus arrhythmia. RR amplitude fluctuations vary within 10%.
- Sinus bradycardia. PQ \u003d 12 seconds, heart rate less than 60 bpm.
- Tachycardia. Heart rate in adolescents is more than 200 beats / min, in adults - more than 100-180. During ventricular tachycardia, the QRS index is higher than 0.12 seconds, sinus tachycardia - slightly exceeds the norm.
- Extrasystoles. An extraordinary contraction of the heart is permissible in isolated cases.
- Paroxysmal tachycardia. An increase in the number of heartbeats up to 220 per minute. Fusion of QRS and P is observed during an attack. Range between R and P from next contraction
- Atrial fibrillation. The contraction of the atria is equal to 350-700 per minute, of the ventricles - 100-180 per minute, P is absent, fluctuations along the isoline.
- Atrial flutter. Atrial contraction is equal to 250-350 per minute, gastric contractions become less frequent. Sawtooth waves in branches ΙΙ-and V1.
EOS position deviation
A displacement of the EOS vector may indicate health problems:
- Deviation to the right is more than 90º. In combination with the excess of the height S over R, it signals pathologies of the right ventricle and a blockage of the His bundle.
- Deviation to the left by 30-90º. With a pathological ratio of the heights of S and R - left ventricular hypertrophy, bundle branch block.
Deviations in the position of the EOS can signal the following diseases:
- heart attack;
- pulmonary edema;
- COPD (chronic obstructive pulmonary disease).
Violation of the conducting system
The conclusion of the ECG may include the following pathologies of the conducting function:
- AV block Ι degree - the distance between the P and Q teeth exceeds an interval of 0.2 seconds, the sequence of the path looks like this - P-Q-R-S;
- AV block ΙΙ degree - PQ displace QRS (Mobitz type 1) or QRS falls out along the length of PQ (Mobitz type 2);
- complete AV block - the frequency of atrial contractions is greater than that of the ventricles, PP \u003d RR, PQ length is different.
Certain heart diseases
A detailed interpretation of the electrocardiogram can show the following pathological conditions:
| Disease | ECG manifestations |
| Cardiomyopathy |
|
| Mitral stenosis |
|
| Mitral valve prolapse |
|
| Chronic lung obstruction |
|
| CNS damage |
|
| Hypothyroidism |
|
Video
In the video course "EKG under the power of everyone", cardiac arrhythmias are considered. Taken from the MEDFORS channel.
A simple and straightforward truth or briefly about the global predictor Supreme predictor
What demons are called succubi and incubi What does a succubus look like
The true story of the petrified girl Zoe with the icon of nicholas the wonderworker
Every family has its own demons
Valerian and cats: how does valerian in different forms affect an animal, can it be given to a cat?