 Truth is a mistake that we temporarily believe is correct. ... ...
Truth is a mistake that we temporarily believe is correct. ... ...

 "Yellow-green water" (Russian) Grun. Star (German) Glaucoma (French, English) Jaskra (p ol.) "Blakitna Water" (Ukrainian)
"Yellow-green water" (Russian) Grun. Star (German) Glaucoma (French, English) Jaskra (p ol.) "Blakitna Water" (Ukrainian)
 Glaukomas - owl-eyed Heinrich Schliemann (Troy)
Glaukomas - owl-eyed Heinrich Schliemann (Troy)
 BACKGROUND Avicenna (980-1037), having begun to heal at the age of 18, described glaucoma a thousand years ago. ... ... at the turn of the 1st millennium In his "Canon of Medicine", republished in 1994, there is a description of an eye disease - "cold inflammation" associated with a violation of body fluids
BACKGROUND Avicenna (980-1037), having begun to heal at the age of 18, described glaucoma a thousand years ago. ... ... at the turn of the 1st millennium In his "Canon of Medicine", republished in 1994, there is a description of an eye disease - "cold inflammation" associated with a violation of body fluids
 1000 years ago - Avicenna There is a type of inflammation of the eyes, which has periods and seizures, periods of change in matter and periods of time of its formation. The sludge of pain during inflammation of the eye depends either on the burning juice, which eats away at the membranes, or on the abundance of juice, which stretches them. The substances causing inflammation of the eyes come either from the body in general, or from the head or from the vessels that bring bad matter to the eye, and sometimes bad juices are in the eye itself.
1000 years ago - Avicenna There is a type of inflammation of the eyes, which has periods and seizures, periods of change in matter and periods of time of its formation. The sludge of pain during inflammation of the eye depends either on the burning juice, which eats away at the membranes, or on the abundance of juice, which stretches them. The substances causing inflammation of the eyes come either from the body in general, or from the head or from the vessels that bring bad matter to the eye, and sometimes bad juices are in the eye itself.

 worldwide: 7. 8 million people who are blind in both eyes with glaucoma. According to the International Society of Glaucomatology for 2008
worldwide: 7. 8 million people who are blind in both eyes with glaucoma. According to the International Society of Glaucomatology for 2008
 Incidence rates Statistical studies show that 1 in 200 over 40 years old in the general population suffers from open-angle glaucoma. The general prevalence of the population in this age group is 1.5%. The number of patients increases with age and reaches 12% in the group over 80 years old.
Incidence rates Statistical studies show that 1 in 200 over 40 years old in the general population suffers from open-angle glaucoma. The general prevalence of the population in this age group is 1.5%. The number of patients increases with age and reaches 12% in the group over 80 years old.
 In the general population, the primary OAG is slightly less than 1%. Today in Russia there are more than 500 thousand patients with glaucoma, in the USA the number of patients with POAG is 2.47 million (out of a total of 276.6 million people). According to the American Academy of Ophthalmologists (1996) 116,000 Americans are blinded as a result of glaucoma Incidence rates
In the general population, the primary OAG is slightly less than 1%. Today in Russia there are more than 500 thousand patients with glaucoma, in the USA the number of patients with POAG is 2.47 million (out of a total of 276.6 million people). According to the American Academy of Ophthalmologists (1996) 116,000 Americans are blinded as a result of glaucoma Incidence rates
 In the United States blind in both eyes 4% of the white population 8% of the Negroid race Blind in one eye 8% of the white population 16% of the Black population. The rate of blindness with OAG in European countries averages 12% of all cases of blindness.
In the United States blind in both eyes 4% of the white population 8% of the Negroid race Blind in one eye 8% of the white population 16% of the Black population. The rate of blindness with OAG in European countries averages 12% of all cases of blindness.

 Varianti of the width of the KPC (Shaffer, Nesterov) 4 3 2 1 0 45 o 35 o 20 o 10 o
Varianti of the width of the KPC (Shaffer, Nesterov) 4 3 2 1 0 45 o 35 o 20 o 10 o
 Anatomical and physiological features of the drainage system of the eye Drainage system tissues are avascular Their metabolism is provided by aqueous humor Trabecula contains an array of endothelial cells covering collagen fibers Free radicals and lipid peroxidation products are formed in cells during metabolic processes, which pass to the trabecula and damage it
Anatomical and physiological features of the drainage system of the eye Drainage system tissues are avascular Their metabolism is provided by aqueous humor Trabecula contains an array of endothelial cells covering collagen fibers Free radicals and lipid peroxidation products are formed in cells during metabolic processes, which pass to the trabecula and damage it

 Ethiological classification of glaucoma (D. Vaughan, T. Asbury, P. Riordan-Eva, 1999) A. Primary glaucoma 1. Vidkritokutova a. Primary vidkritokutova glaucoma b. Glaucoma in a normal (low) grip 2. Zakritokutova a. gostra b. підгостра в. chronic V. Vrodzhena glaucoma 1. Primary congenital glaucoma 2. Congenital glaucoma with an underlying pathology of the eye 3. Congenital glaucoma with ocular pathology C. Secondary glaucoma 1. Pigmental 2. Exfoliant syndrome 5 Iridocorneoendothelial syndrome 6. Traumatic 7. Pislyoperative 8. Neovascular 9. Dislocations episcleral venous vise 10. Steroid D. Absolute glaucoma.
Ethiological classification of glaucoma (D. Vaughan, T. Asbury, P. Riordan-Eva, 1999) A. Primary glaucoma 1. Vidkritokutova a. Primary vidkritokutova glaucoma b. Glaucoma in a normal (low) grip 2. Zakritokutova a. gostra b. підгостра в. chronic V. Vrodzhena glaucoma 1. Primary congenital glaucoma 2. Congenital glaucoma with an underlying pathology of the eye 3. Congenital glaucoma with ocular pathology C. Secondary glaucoma 1. Pigmental 2. Exfoliant syndrome 5 Iridocorneoendothelial syndrome 6. Traumatic 7. Pislyoperative 8. Neovascular 9. Dislocations episcleral venous vise 10. Steroid D. Absolute glaucoma.
 Clinical classification developed by A.P. Nesterov and A. Ya. Bunin and adopted at the III All-Russian Congress of Ophthalmologists (1975). ACUTE GLAUCOMA Form of glaucoma Stage IOP state Dynamics of visual function Angle-closure Open-angle Initial I Developed II Unstabilized Stabilized. Normal (A) Moderately high (B) Far-reaching III High (C) Mixed Terminal IV
Clinical classification developed by A.P. Nesterov and A. Ya. Bunin and adopted at the III All-Russian Congress of Ophthalmologists (1975). ACUTE GLAUCOMA Form of glaucoma Stage IOP state Dynamics of visual function Angle-closure Open-angle Initial I Developed II Unstabilized Stabilized. Normal (A) Moderately high (B) Far-reaching III High (C) Mixed Terminal IV



 Hereditary form of congenital glaucoma - an autosomal recessive disease, which is based on underdevelopment of the drainage zone of the eye
Hereditary form of congenital glaucoma - an autosomal recessive disease, which is based on underdevelopment of the drainage zone of the eye
 Causes of Congenital Glaucoma Unabsorbed embryonic tissue in the corner of the anterior chamber Anterior attachment of the iris root Underdevelopment of the trabecula Absence of the helmet canal Underdevelopment of the intrascleral outflow tract
Causes of Congenital Glaucoma Unabsorbed embryonic tissue in the corner of the anterior chamber Anterior attachment of the iris root Underdevelopment of the trabecula Absence of the helmet canal Underdevelopment of the intrascleral outflow tract
 Clinical signs of congenital glaucoma Photophobia, blepharospasm, lacrimation Increase in the size of the cornea (from 9 to 22 mm) Edema, swelling, opacity of the cornea. Ruptures of Descemet's sheath Expansion of the limbus (from 1 mm to 3-4 mm) Staple sclera Increase in the size of the eyeball (from 16 to 35 mm) Changes in the structures of the UPC> IOP Glaucomatous excavation
Clinical signs of congenital glaucoma Photophobia, blepharospasm, lacrimation Increase in the size of the cornea (from 9 to 22 mm) Edema, swelling, opacity of the cornea. Ruptures of Descemet's sheath Expansion of the limbus (from 1 mm to 3-4 mm) Staple sclera Increase in the size of the eyeball (from 16 to 35 mm) Changes in the structures of the UPC> IOP Glaucomatous excavation




 OBJECTIVE CHANGES IN OAG (in the advanced and late stages of the disease) Symptom of emisaria Symptom of cobra Pathological pigmentation of the UPC Dispersion of the iris pigment Atrophy of the iris stroma Leaching of the pigment border Presence of pseudoexfoliation Glaucomatous field of the optic nerve disc changes in the hydrodynamic changes
OBJECTIVE CHANGES IN OAG (in the advanced and late stages of the disease) Symptom of emisaria Symptom of cobra Pathological pigmentation of the UPC Dispersion of the iris pigment Atrophy of the iris stroma Leaching of the pigment border Presence of pseudoexfoliation Glaucomatous field of the optic nerve disc changes in the hydrodynamic changes
 Clinic of glaucoma: Occurs and progresses imperceptibly Absence of pain and discomfort Complaints about the periodic appearance of rainbow circles blurred vision, sometimes headache in the brow region
Clinic of glaucoma: Occurs and progresses imperceptibly Absence of pain and discomfort Complaints about the periodic appearance of rainbow circles blurred vision, sometimes headache in the brow region

 Risk factors for an acute attack of glaucoma Nervous tension Overwork Staying in the dark Medicamental mydriasis Prolonged head tilts Stress Drinking lots of fluids
Risk factors for an acute attack of glaucoma Nervous tension Overwork Staying in the dark Medicamental mydriasis Prolonged head tilts Stress Drinking lots of fluids
 The scheme of development of an acute attack of glaucoma. C hart T itle O s t u r s t u p gl a c o m Full block Offset e r i d o x r u s t a l and k o w o y d i a f r a g m o T e x te c l o v and d o f body O C u s i i y t r a b ekular z o n s B o m b a j r and o n s a l e r a n s in the back c a m e r S h e n g e t o c in g z f u nk ts i on al block c m e c e n i e r i d about x rust a l and k o w o y d i a f r a g m s
The scheme of development of an acute attack of glaucoma. C hart T itle O s t u r s t u p gl a c o m Full block Offset e r i d o x r u s t a l and k o w o y d i a f r a g m o T e x te c l o v and d o f body O C u s i i y t r a b ekular z o n s B o m b a j r and o n s a l e r a n s in the back c a m e r S h e n g e t o c in g z f u nk ts i on al block c m e c e n i e r i d about x rust a l and k o w o y d i a f r a g m s
 links of glaucoma pathogenesis Specific atrophy of the optic nerve head with excavation. Impaired hemodynamics in the optic nerve system OPTICAL NEUROPATHY decreased perfusion Impaired autoregulation increased IOP apoptosis
links of glaucoma pathogenesis Specific atrophy of the optic nerve head with excavation. Impaired hemodynamics in the optic nerve system OPTICAL NEUROPATHY decreased perfusion Impaired autoregulation increased IOP apoptosis
 Control of IOP IOP - pressure of the contents of the eyeball on its walls Function of rigidity of the eye and its volume Depends on - production of IOP - outflow of IOP - volume of anatomical structures - resistance and blood filling of the eye vessels
Control of IOP IOP - pressure of the contents of the eyeball on its walls Function of rigidity of the eye and its volume Depends on - production of IOP - outflow of IOP - volume of anatomical structures - resistance and blood filling of the eye vessels

















 Volumetric model of normal and pathological differential light sensitivity as a function of localization in the field of view (Bebie. H., Fankhauser F., 1983) "Island of vision"
Volumetric model of normal and pathological differential light sensitivity as a function of localization in the field of view (Bebie. H., Fankhauser F., 1983) "Island of vision"


 Features of glaucoma changes in the visual field Changes in the peripheral visual field in glaucoma. a - narrowing of the visual field from the nasal side, breakthrough of Bjerrum's scotoma to the periphery; b - concentric narrowing; c - tubular field of view; d - residual island of the field of view.
Features of glaucoma changes in the visual field Changes in the peripheral visual field in glaucoma. a - narrowing of the visual field from the nasal side, breakthrough of Bjerrum's scotoma to the periphery; b - concentric narrowing; c - tubular field of view; d - residual island of the field of view.
 In the first stage, a relative arcuate defect is revealed. Isopter depression is often detected in the region from 5 to 25 degrees. from the fixation point, it is possible to identify a small scotoma in the same area. Five stages of development of glaucomatous visual field defects (Authorn, 1978) I
In the first stage, a relative arcuate defect is revealed. Isopter depression is often detected in the region from 5 to 25 degrees. from the fixation point, it is possible to identify a small scotoma in the same area. Five stages of development of glaucomatous visual field defects (Authorn, 1978) I
 In the second stage, the appearance of deep defects of a round shape is noted, or by cattle that do not merge with the blind spot, they are often detected in the nasal region and an increase in the size of the blind spot. Five stages of development of glaucomatous visual field defects (Authorn, 1978) II
In the second stage, the appearance of deep defects of a round shape is noted, or by cattle that do not merge with the blind spot, they are often detected in the nasal region and an increase in the size of the blind spot. Five stages of development of glaucomatous visual field defects (Authorn, 1978) II
 In the third stage, an arcuate scotoma appears, often with a breakthrough to the periphery in the nasal region, which leads to the formation of the classic nasal step. Five stages of development of glaucomatous visual field defects (Authorn, 1978) ІІІ
In the third stage, an arcuate scotoma appears, often with a breakthrough to the periphery in the nasal region, which leads to the formation of the classic nasal step. Five stages of development of glaucomatous visual field defects (Authorn, 1978) ІІІ
 In the fourth stage, a widespread circular or semicircular scotoma may appear, leaving an island of vision in the center, as well as peripheral vision. Five stages of development of glaucomatous visual field defects (Authorn, 1978) I V
In the fourth stage, a widespread circular or semicircular scotoma may appear, leaving an island of vision in the center, as well as peripheral vision. Five stages of development of glaucomatous visual field defects (Authorn, 1978) I V
 In the fifth stage, the center of the visual hill practically collapses and only residual vision from the temporal side remains. Five stages of development of glaucomatous visual field defects (Authorn, 1978) V
In the fifth stage, the center of the visual hill practically collapses and only residual vision from the temporal side remains. Five stages of development of glaucomatous visual field defects (Authorn, 1978) V





 The number of capillaries in the ethmoid plate layer is 3300. 1 axon bundle is supplied with blood by 8 capillaries. There are 2500 capillaries in 1 mm of the optic nerve; 1 capillary supplies 312 axons with blood. Biological vulnerability of the optic nerve
The number of capillaries in the ethmoid plate layer is 3300. 1 axon bundle is supplied with blood by 8 capillaries. There are 2500 capillaries in 1 mm of the optic nerve; 1 capillary supplies 312 axons with blood. Biological vulnerability of the optic nerve
 Biological vulnerability of the optic nerve lack of capillaries inside the bundles of optic nerve axons inadequate blood supply to axons decrease in the partial pressure of oxygen in post-capillary venules disproportion between the length of the axon (15 cm) and its thickness (15 mm)
Biological vulnerability of the optic nerve lack of capillaries inside the bundles of optic nerve axons inadequate blood supply to axons decrease in the partial pressure of oxygen in post-capillary venules disproportion between the length of the axon (15 cm) and its thickness (15 mm)
 Biological vulnerability of the optic nerve extreme compression of axons in the ethmoid plate absence of myelin sheath absence of lymphatic capillaries in the optic nerve lack of sensory innervation in the optic nerve
Biological vulnerability of the optic nerve extreme compression of axons in the ethmoid plate absence of myelin sheath absence of lymphatic capillaries in the optic nerve lack of sensory innervation in the optic nerve
 Anatomy of the optic disc blood supply The main source is the posterior short ciliary arteries on the left of the figure [according to Cioffi, van Buskrik, 1996].
Anatomy of the optic disc blood supply The main source is the posterior short ciliary arteries on the left of the figure [according to Cioffi, van Buskrik, 1996].
 Quantitative criteria for the stage of glaucoma with uniform expansion of the visible zone of axonal atrophy in all directions (type I excavation), if E / D is:< 0, 4 — преглаукома; 0, 4 — 0, 5 — начальная глаукома; 0, 6 — 0, 7 — развитая глаукома; 0, 8 — 0, 9 — далеко зашедшая стадия. Достоверность показателей верифицируется меньшими размерами экскавации на парном глазу и наличием характерных для глаукомы нарушений зрения:
Quantitative criteria for the stage of glaucoma with uniform expansion of the visible zone of axonal atrophy in all directions (type I excavation), if E / D is:< 0, 4 — преглаукома; 0, 4 — 0, 5 — начальная глаукома; 0, 6 — 0, 7 — развитая глаукома; 0, 8 — 0, 9 — далеко зашедшая стадия. Достоверность показателей верифицируется меньшими размерами экскавации на парном глазу и наличием характерных для глаукомы нарушений зрения:

 The approximate forms of recording and sketching data of optic disc ophthalmoscopy in the presence of signs of glaucoma are as follows. Example 1. Slight deflection of the temporal half of the optic disc of the left eye with a sector of atrophy within one (inferior temporal) quadrant with moderate thinning of the IU with the presence of a beta zone in the sector of atrophy of the disc with a width of about 0.1 (to the diameter of the disc). No hemorrhages.
The approximate forms of recording and sketching data of optic disc ophthalmoscopy in the presence of signs of glaucoma are as follows. Example 1. Slight deflection of the temporal half of the optic disc of the left eye with a sector of atrophy within one (inferior temporal) quadrant with moderate thinning of the IU with the presence of a beta zone in the sector of atrophy of the disc with a width of about 0.1 (to the diameter of the disc). No hemorrhages.
 The approximate forms of recording and sketching data of optic disc ophthalmoscopy in the presence of signs of glaucoma are as follows. Example 2. Barely noticeable total deflection of the optic nerve disc of the right eye, emphasized by the course of the vessels, with a rounded area of pallor in the center of size E / D 0, 7. In the meridian 7 hours along the edge of the disc, streaky hemorrhage.
The approximate forms of recording and sketching data of optic disc ophthalmoscopy in the presence of signs of glaucoma are as follows. Example 2. Barely noticeable total deflection of the optic nerve disc of the right eye, emphasized by the course of the vessels, with a rounded area of pallor in the center of size E / D 0, 7. In the meridian 7 hours along the edge of the disc, streaky hemorrhage.
 The approximate forms of recording and sketching data of optic disc ophthalmoscopy in the presence of signs of glaucoma are as follows. Example 3. The optic nerve disc of the left eye in the entire temporal half with a transition below to a part of the nasal half of a grayish-white color, excavated. The zones of depression and blanching coincide. In the long run (in the sector more than 6 hours), the IU is completely absent. The adjacent beta zone reaches a width of 0.3 (to the diameter of the disc).
The approximate forms of recording and sketching data of optic disc ophthalmoscopy in the presence of signs of glaucoma are as follows. Example 3. The optic nerve disc of the left eye in the entire temporal half with a transition below to a part of the nasal half of a grayish-white color, excavated. The zones of depression and blanching coincide. In the long run (in the sector more than 6 hours), the IU is completely absent. The adjacent beta zone reaches a width of 0.3 (to the diameter of the disc).
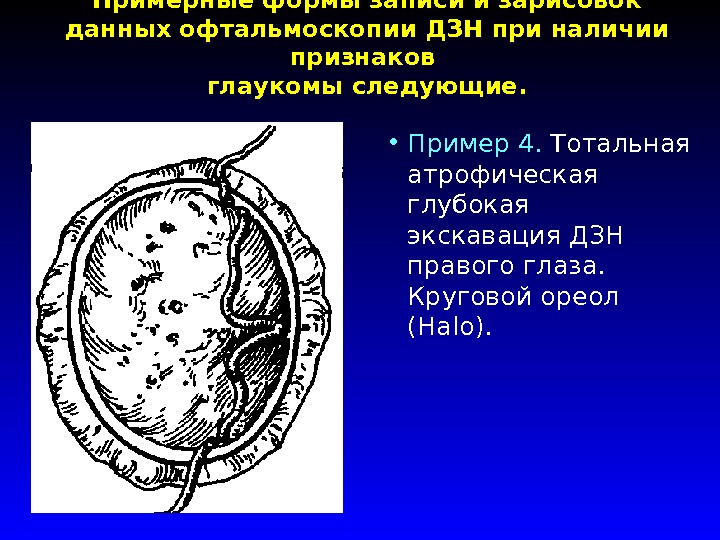 The approximate forms of recording and sketching data of optic disc ophthalmoscopy in the presence of signs of glaucoma are as follows. Example 4. Total atrophic deep excavation of the optic nerve disc of the right eye. Circular halo (Halo).
The approximate forms of recording and sketching data of optic disc ophthalmoscopy in the presence of signs of glaucoma are as follows. Example 4. Total atrophic deep excavation of the optic nerve disc of the right eye. Circular halo (Halo).

Slide 1
GRODNO STATE MEDICAL UNIVERSITY DEPARTMENT OF OTORINOLARYNGOLOGY, OPHTHALMOLOGY AND DENTAL LECTURE No. 5 Glaucoma. Clinic, diagnostics, treatment, prevention of glaucoma. Lecturer: Assoc. S. N. IlyinaSlide 2
 Glaucoma - a disease EYE, characterized by: continuously or intermittently elevated intraocular pressure, characteristic changes in the field of vision, decreased visual acuity of central vision, excavation optic nerve and blindness ZAKANCHIVYUSCHEESYA THE ABSENCE MANAGEMENT TREATMENT 3% of patients treated at the reception 20% BLIND DUE TO LOSE SIGHT glaucoma
Glaucoma - a disease EYE, characterized by: continuously or intermittently elevated intraocular pressure, characteristic changes in the field of vision, decreased visual acuity of central vision, excavation optic nerve and blindness ZAKANCHIVYUSCHEESYA THE ABSENCE MANAGEMENT TREATMENT 3% of patients treated at the reception 20% BLIND DUE TO LOSE SIGHT glaucoma
Slide 3

Slide 4
 I. COMPLAINTS SENSE OF PRESSURE IN THE EYES FEELING OF “TEARS”, OF A FOREIGN BODY “BLACK FLIES” IN FRONT OF EYES PHOTOSES EARLY PRESBIOPIA II. DETERMINATION OF IOP TONOMETRY ACCORDING TO MAKLAKOV AND DAILY TONOMETRY ELASTOTONOMETRY TONOGRAPHY PALPATORNO III. STUDY OF THE ANGLE OF THE FRONT CAMERA GONIOSCOPY WURGAFT METHOD IV. PERIPHERAL VISION STUDY CAMPIMETRY PERIMETRY V. BIOMICROSCOPY AND OPHTHALMOSCOPY
I. COMPLAINTS SENSE OF PRESSURE IN THE EYES FEELING OF “TEARS”, OF A FOREIGN BODY “BLACK FLIES” IN FRONT OF EYES PHOTOSES EARLY PRESBIOPIA II. DETERMINATION OF IOP TONOMETRY ACCORDING TO MAKLAKOV AND DAILY TONOMETRY ELASTOTONOMETRY TONOGRAPHY PALPATORNO III. STUDY OF THE ANGLE OF THE FRONT CAMERA GONIOSCOPY WURGAFT METHOD IV. PERIPHERAL VISION STUDY CAMPIMETRY PERIMETRY V. BIOMICROSCOPY AND OPHTHALMOSCOPY
Slide 5

Slide 6

Slide 7

Slide 8
 I. PRIMARY 1. FRONT CAMERA ANGLE STATUS - OPEN ANGLE - CLOSED ANGLE - MIXED 2. DEVELOPMENT STAGES - INITIAL - DEVELOPED - FAR PREST - TERMINAL 3. PRESENT - EXTREMELY 28 mm - NORMALLY 27 mm - HIGH (OVER 32 mm) DYNAMICS OF VISUAL FUNCTIONS - STABILIZED - UNSTABILIZED II. SECONDARY III. Congenital IV. JUVENILE
I. PRIMARY 1. FRONT CAMERA ANGLE STATUS - OPEN ANGLE - CLOSED ANGLE - MIXED 2. DEVELOPMENT STAGES - INITIAL - DEVELOPED - FAR PREST - TERMINAL 3. PRESENT - EXTREMELY 28 mm - NORMALLY 27 mm - HIGH (OVER 32 mm) DYNAMICS OF VISUAL FUNCTIONS - STABILIZED - UNSTABILIZED II. SECONDARY III. Congenital IV. JUVENILE
Slide 9
 I. OPEN-ANGLE GLAUCOMA FLOWS INSIDERABLY INTRAOCULAR PRESSURE INCREASED (NOT ALWAYS) PROGRESSIVE CONSTRUCTION OF THE VISUAL FIELD EXCAVATION OF THE POPULAR NERVE OPEN ANGLE OF THE ANTERIOR CAMERA II. CLOSE-ANGLE GLAUCOMA FLOWS INSERT, EYE PAINS HORRAL SENSITIVITY REDUCED CORNAL SENSITIVITY CONSTANT INJECTION SMALL FRONT CHAMBER ANTERIOR CORNER CORNER CORNER
I. OPEN-ANGLE GLAUCOMA FLOWS INSIDERABLY INTRAOCULAR PRESSURE INCREASED (NOT ALWAYS) PROGRESSIVE CONSTRUCTION OF THE VISUAL FIELD EXCAVATION OF THE POPULAR NERVE OPEN ANGLE OF THE ANTERIOR CAMERA II. CLOSE-ANGLE GLAUCOMA FLOWS INSERT, EYE PAINS HORRAL SENSITIVITY REDUCED CORNAL SENSITIVITY CONSTANT INJECTION SMALL FRONT CHAMBER ANTERIOR CORNER CORNER CORNER
Slide 10
 I. OPTOCULAR GLAUKOMA - MEDICINAL TREATMENT PILOCARPINE β-BLOCKERS (THIMOLOL, OPTIMOL, ARUTIMOL) TRAVATAN, XALATAN AZOPT, TRUSOPT ANTIOXIDANTS VASCULAR PREHYDRACES II CLOSED-ANGLE GLAUKOMA SURGICAL TREATMENT: SYNUSTRABECULECTOMY
I. OPTOCULAR GLAUKOMA - MEDICINAL TREATMENT PILOCARPINE β-BLOCKERS (THIMOLOL, OPTIMOL, ARUTIMOL) TRAVATAN, XALATAN AZOPT, TRUSOPT ANTIOXIDANTS VASCULAR PREHYDRACES II CLOSED-ANGLE GLAUKOMA SURGICAL TREATMENT: SYNUSTRABECULECTOMY
Slide 11
 I. COMPLAINTS IRRADIATING HEADACHE REDUCED VISUALITY RAIN CIRCLES WHEN LOOKING AT THE SOURCE OF LIGHT II. OBJECTIVELY CONSISTENT INJECTION CORNEAL Edema SMALL FRONT CAMERA WIDE IOP Pupil INCREASED UP TO 40-50 mm. rt. Art. III. TREATMENT: CONSERVATIVE UP TO 12-24 HOURS FROM THE MOMENT OF THE ATTACK. IF IOP DOES NOT DECREASE - IRIDECTOMIA. IN PLANNED ORDER - TRABECULECTOMY.
I. COMPLAINTS IRRADIATING HEADACHE REDUCED VISUALITY RAIN CIRCLES WHEN LOOKING AT THE SOURCE OF LIGHT II. OBJECTIVELY CONSISTENT INJECTION CORNEAL Edema SMALL FRONT CAMERA WIDE IOP Pupil INCREASED UP TO 40-50 mm. rt. Art. III. TREATMENT: CONSERVATIVE UP TO 12-24 HOURS FROM THE MOMENT OF THE ATTACK. IF IOP DOES NOT DECREASE - IRIDECTOMIA. IN PLANNED ORDER - TRABECULECTOMY.
GBOU RM SPO (SSUZ)"Saransk Medical College"
Methodical development
on an open theoretical lesson on the topic:
« Violations of the hydrodynamics of the eye. Etiology, clinical manifestations, treatment. Emergency care for an acute attack of glaucoma "
Item - Eye diseases
Speciality - Medicine
Qualification - paramedic
The level of education - increased
Performed by prep. Shamshetdinova G.Kh.
Saransk 2012
Explanatory note
This lesson is devoted to the most pressing topic of our time, glaucoma. NSaccording to literature data (including WHO), the number of glaucoma patients in the world reaches 100 million people. Glaucoma ranks first among the causes of visual disability.
The methodological development is intended for the training of paramedical workers in the specialty "General Medicine", qualification "Paramedic" (advanced level of education) in the subject "Eye Diseases".
This lesson is theoretical and is conducted in accordance with the lecture plan. To facilitate the perception of the lecture material, a multimedia illustration is used in the lesson.
In the lesson, in order to better perceive the material, fragments of the techniques are used:critical thinking technology (compilation of clusters and syncwines), which allowsorganizedbeprocesslearningaimed at vigorous activity on the comprehension, application, analysis, generalization or evaluation of information obtained or created through observation, experience, reflection, reasoning or communication as a guide to action or the formation of a belief; case method allowingconsolidate the knowledge gained in previous lessons,to work out the skills of the practical use of conceptual schemes and to familiarize students with schemes for the analysis of practical situations, as well as to work out the skills of group analysis of problems and decision-making (within the framework of training procedures);health saving technologies anddevelopmental learning technologies .
To control and consolidate the knowledge gained at the end of the lesson, situational tasks are carried out. Much attention is paid to the independent work of students, it was proposed to prepare short messages, reflecting their opinion on the topic under consideration.
Tasks:
1. To study the anatomical and physiological features and functions of the visual analyzer, their changes in glaucoma.
2. To study the research methods used in the diagnosis of glaucoma.
3. To study the clinical manifestations of glaucoma.
4. To study emergency care in acute and subacute attacks of glaucoma and the tactics of managing a patient with glaucoma.
5. To study the rules of dispensary observation of glaucoma patients.
The purpose of the lesson:
Educational - to study the concept of etiopathogenesis, clinical manifestations, principles of glaucoma treatment.
Developing - to promote the development of clinical thinking, memory, attention; instill the ability to work with educational and technical literature.
Upbringing - to promote the upbringing of industriousness, accuracy, a sense of responsibility and honesty, to influence the aesthetic views of students, to contribute to the formation of professional qualities in the work of a paramedic.
Interdisciplinary connections:
anatomy;
physiology;
therapy;
obstetrics;
pediatrics;
psychology.
Duration of the lesson:
1. Organizational moment: checking the attendance of students, checking the readiness for the lesson, announcing the topic of the lesson, objectives and goals of the lesson, the introductory word of the teacher - the motivation of the lesson - 5 min.
2. Presentation of new material - 50 min.
2.1 Presentation of the material - 25 min.
2.2 Physical education - 3-5 minutes.
2.3 Presentation of the material - 20 min.
3. Messages from students - 15 min.
4. Consolidation of material (compilation of clusters, syncwines, situational tasks) - 15 min.
5. Summing up - 5 min .________________________________
Total: 90 min.
The course of the lesson.
1 Introductory word (5 minutes).
This lesson is devoted to a topical topic of our time, namely, the disease, which ranks first among the causes of blindness and disability in terms of the organ of vision, glaucoma.From 1% to 2% of the population over 40 years old is affected by this ailment.According to the WHO, there are more than 100 million patients with glaucoma in the world, and their number is steadily increasing every year. This number is forecast to double by 2030.
Even at the level of modern knowledge, it remains unclear what is the impetus for the occurrence of glaucoma. Many diseases inherent in old age contribute to its development. These include diseases of the cardiovascular system (atherosclerosis, hypertension), the endocrine system (diabetes mellitus, thyroid disease), and the nervous system.
A hereditary factor plays a huge role in the occurrence of glaucoma. It is 35%. Blood relatives of patients with glaucoma constitute the main risk group and must undergo a preventive eye examination every year.
2 Presentation of new material (50 minutes):
Glaucoma - a large group of eye diseases, each of which is characterized by a constant or periodic increase in intraocular pressure caused by a violation of the outflow of aqueous humor from the eye, as a result, a special form of optic nerve atrophy with excavation in the disc area develops. It is characterized by a triad of signs:
1 increase in intraocular pressure.
2 progressive glaucomatous optic atrophy.
3 progressive decrease in central and peripheral vision.
Etiological factors occurrence of glaucoma: heredity, metabolic disorders, hemodynamic and endocrine disorders, local dystrophic changes.
Classification:
By origin: primary, secondary and combined with defects in the development of the eye and other structures.
According to the patient's age: congenital, infantile, juvenile and adult glaucoma.
By the mechanism of increasing intraocular pressure: open-angle, closed-angle, dysgenesis of the anterior chamber angle, pretrabecular block and peripheral block.
By IOP level: hypertensive and normotensive.
According to the degree of damage to the optic nerve head: initial, developed, distant and terminal.
Adrift: stable and unstable.
Pathogenesis associated with a violation of the outflow of aqueous humor - with the development of trabeculopathy and functional canalicular block, and is common to all forms of primary open-angle glaucoma. Violation of the hydrodynamics of the eye leads to an increase in IOP above the normal level and the development of optic nerve disc atrophy of the glaucoma type.
Congenital glaucoma.
The cause of congenital glaucoma is unabsorbed embryonic mesodermal tissue, anterior attachment of the iris, - dysgenesis of the UPC, leading to obstruction of the outflow of aqueous humor, and then to an increase in IOP.
Clinic. Congenital glaucoma is characterized by an imperceptible course. You can suspect glaucoma due to a small photophobia, lacrimation, restless behavior, and a child's sleep. The cornea, the anterior chamber of the eye and the pupil increase in size. The cornea may appear as "misted" glass or white porcelain. This type of it is most often caused by edema or already dystrophy of the cornea.
Edema can be distinguished from dystrophy when one of the hypertonic solutions (glucose, urea, glycerin, and even saline) is instilled into the cornea: the edema disappears or decreases after instillation. But not only the size of the cornea can be increased by about 11 mm (not 9 mm), the depth of the anterior chamber is 3-4 mm (not 2 mm), the width of the pupil is 3-4 mm (not 2 mm), but also the entire eyeball , and this increase reflects the stage of the glaucomatous process.
An enlargement of the entire eye is the so-called buphthalmos (bull's eye) or hydrophthalmos (dropsy of the eye). A high ophthalmotonus is also evidenced by the presence of a stagnant injection of the eye with the characteristic symptoms of "emissary", "cobra head", an othoracic "jellyfish body". The magnitude of the increase in intraocular pressure is determined by palpation as T + 2 and even higher (T + 3).
If the cornea is transparent, then with ophthalmoscopy, in the area of the disc (nipple) of the optic nerve, a shift of the vascular bundle to the nasal side and pathological atrophic excavation of the disc itself can be detected.
All of the listed glaucomatous changes in various structures of the eye cannot but affect visual functions: they are reduced, respectively, by the stage of the process and the severity of symptoms.
Treatment: Surgical - goniotomy operation. The purpose of the goniotomy is to destroy the mesodermal tissue in the corner of the anterior chamber and open the outflow of moisture in the anterior chamber through the Schlemm canal; or goniotonia with goniopuncture - + creation of an additional outflow of intraocular fluid under the conjunctiva
If help is not provided - atrophy of the optic nerve, by the year the eye will go blind.
Open angle glaucoma accounts for more than 90% of all cases of this disease. In this form of glaucoma, the iris-corneal angle is open, which is why its name. For reasons not yet fully understood, the outflow of intraocular fluid is impaired. This leads to its accumulation and a gradual but constant increase in pressure, which can ultimately destroy the optic nerve and cause loss of vision.
In most casesopen-angle glaucoma arises and progresses imperceptibly for a patient who does not experience any unpleasant sensations and turns to a doctor already at a late stage of the disease, when he notices a deteriorationvisual acuity... Appearance complaintsrainbow circlesaround light sources, periodicblurred vision note only 15-20% of patients. It is these symptoms that appear with an increaseand may be accompanied by pain in the brow region and head.
Open angle glaucoma affects, as a rule, both eyes, in most cases, flowing asymmetrically.
The leading symptom of the disease is an increaseintraocular pressure (IOP) . Intraocular pressure at open-angle glaucoma rises slowly and gradually as the outflow resistance builds upintraocular fluid (IVF) ... In the initial period, it is fickle, then it becomes persistent.
The most important diagnostic featureopen-angle glaucoma is the changefield of view... First of all, these defects are determined in the central sections and are manifested by the expansion of the boundaries of the blind spot, the appearance of arcuate prolapse. These disorders are detected early.glaucoma, with special studiesvisual fields... As a rule, the patients themselves do not notice these changes in their daily life.
With further developmentglaucomatous process come to light peripheral visual field defects ... Constriction field of viewoccurs mainly from the nasal side, further narrowing of the field of view concentrically covers the peripheral parts up to its complete loss. Dark adaptation is deteriorating. These symptoms appear against the background of a persistent increase inintraocular pressure (IOP) ... The fall visual acuityspeaks already of a severe, advanced stage of the disease, accompanied by an almost completeoptic atrophy .
Closed-angle glaucoma - a more rare form of glaucoma. Women get sick more often than men. Predisposing factors for the development of this formglaucoma are:
anatomical predisposition;
functional closure factorsanterior chamber angle ;
age-related changes in the eye.
Anatomical structural featureseyeball predisposing to developmentangle-closure glaucoma small eye size, small anterior chamber, largelens , narrowanterior chamber angle , hyperopia ... Functional factors include increased productionintraocular fluid (IVF) , increased blood circulationintraocular vessels , pupil dilation .
In this form of glaucoma, the pressure in the eye rises rapidly. Anything that causes the pupil to dilate, such as dim light, certain medications, and even dilating eye drops used before the eye exam can cause the iris to block the flow of intraocular fluid in some people. When this form of the disease occurs, the eyeball quickly hardens and the sudden pressure causes pain and blurred vision.
Flowangle-closure glaucoma in most patients is characterized by periodic, at first short-term, and then more and more prolonged periods of increaseintraocular pressure (IOP) ... At the initial stage, this is due to the mechanical closure of the zonetrabeculae iris root , which is due to the anatomical predispositions of the eye. Whereinoutflow of intraocular fluid (IVF) decreases. When fully closedanterior chamber angle a condition calledacute attack of angle-closure glaucoma ... In the intervals between attacks, the corner opens.
During such attacks, adhesions are gradually formed between the iris and the wall of the anterior chamber angle, the disease gradually acquires a chronic course with a constant increaseintraocular pressure (IOP) .
Duringangle-closure glaucoma phases such as:
preglaucoma;
acute attack of glaucoma;
chronic course of glaucoma.
Preglaucoma occurs in individuals who do not have clinical manifestations of the disease, but upon examinationanterior chamber angle it is found that it is either narrow or closed. Betweenpregaucoma andacute attack of glaucoma possible transient symptoms of visual discomfort, the appearance of rainbow circles when looking at a light source, short-termloss of sight ... Most often, these phenomena occur with prolonged stay in the dark or emotional arousal (these conditions contribute to the dilation of the pupil, which completely or partially reducesoutflow of intraocular fluid ) and usually disappear on their own, without causing much concern in patients.
Acute attack of glaucoma occurs under the influence of provoking factors, such as nervous tension, overwork, prolonged stay in the dark, drug-induced dilation of the pupil, prolonged work in a tilted position of the head, intake of a large amount of fluid. Sometimes an attack appears for no apparent reason. The patient complains abouteye pain and in the head, especially in the back of the head,nausea, often vomiting, general weakness, blurred vision , the appearance rainbow circles when looking at a light source. An acute attack of glaucoma is often mistaken for migraine, hypertensive crisis, poisoning, which leads to serious consequences, because such a patient must be helped in the first hours of the disease.
Painful sensations are caused by compression of nerve elements inroot of the iris andciliary body ... Visual discomfort is associated with corneal edema.
On visual inspection without special devices, one can notice only a sharp expansion of the vessels on the anterior surface of the eyeball, the eye becomes "red", somewhat bluish (stagnant injection of blood vessels). The cornea becomes cloudy due to the development of edema. Noteworthy is the dilated pupil that does not react to light. At the height of the enacted attack, it can sharply decreasevisual acuity ... Intraocular pressure can rise to 60-80 mm Hg. Art.,outflow of fluid from the eye stops almost completely. The eye is as dense to the touch as a stone.
If, within the next few hours after the onset of the attack, the pressure is not relieved with medication or surgery,to the eye irrevocable threatensloss of sight !!! Acute attack of glaucoma is an urgent situation and requires emergency medical care !!!
Over time, the disease becomes chronic. This typeglaucoma proceeds with a progressive riseintraocular pressure (IOP) , subacute attacks and increasing blockadeanterior chamber angle ... These processes naturally end with developmentglaucomatous optic atrophy , loss of visual function .
Urgent care:
1 instillation of pilocarpine 1% for the first 2 hours every 15 minutes, the next 2 hours. every 30 min., in inc. track. 2 hours 1 time per hour. Further 3-6 r / d from the degree of IOP reduction.
2 0.5% timolol 2r / d.
3 orally or parenterally osmotic diuretics, i / m or i / v-furosemide, 20-40 mg.
4 inside acetazolamide at 0.25-0.5 g 2-3r / d.
5 dorzolamide 2% 3r / d.
6 i / m lytic mixture: 1-2 ml 2.5% aminosine + 1 ml 2% diphenhydramine + 1 ml 2% promedol. After the introduction of the mixture, bed rest for 3-4 hours of professional orthostatic collapse.
7 for relief of an attack and prevention of recurrent attacks - laser iridectomy in both eyes.
8 if the attack could not be stopped within 12-24 hours, surgical treatment is indicated.
Secondary glaucoma is a complication of inflammatory diseases or eye injuries, as a result of which there is an outflow of fluid through the drainage system.
Glaucoma stages:
Initial: the boundaries of the visual field are normal, but there are changes in the paracentral parts of the visual field (individual scotomas in the zone 5-200 , Bjerum's arcuate scotoma, blind spot enlargement). M. b. the initial signs of excavation of the optic nerve head.
Developed: pronounced changes in the visual field in the paracentral region in combination with a narrowing of its peripheral boundaries by more than 100 in the upper or lower nasal segment. Excavation of the optic nerve head approaches the marginal.
Far-reaching: the border of the visual field is concentrically narrowed and in one or more segments is located in less than 150 from the fixation point, there is a marginal excavation of the optic nerve head.
Terminal: complete loss of vision or preservation of light perception with incorrect light projection. The field of view cannot be examined.
IOP level: a - within normal limits (18-24 mm Hg); в-moderately increased (25-32 mm Hg. Art.); c-high pressure (33 mm Hg).
Treatment:
1 drugs of first choice: 1% pilocarpine, 0.25% and 0.5% timolol, 0.005% latanoprost. If the drug is ineffective, it is replaced with another drug of the first choice or a combination of the first and second choice (0.25% and 0.5% betaxolol, 1-2% proxodolol, 2% -dorzolamide)
2 enzymatic antioxidants - superoxide dismutase-Erisod.
3 1% emoxipin subconjunctival and parabulbar 10 injections. The effect of emoxipin is enhanced by its combined use with tocopherol. Aevit 1 caps. 2-3r / d with vitamins gr. V.
4 antispasmodics - inside xanthinol nicotinate 150 mg 3 r / d after meals 2 months. or i / m 15% 2 ml 1 r / d 10 days. Theophylline 250mg 3 r / d 2 weeks; Cavinton 5 mg 3 r / d for 1 month; pentoxifylline after meals 400 mg 3 r / d.
5 angioprotectors - dicinone 0.25g 3r / d 2-3 months; prodectin 0.25g 3-4r / d2-4w
6 nootropic drugs - nootropil 30-160mg / kg / day 6-8 weeks Picamilon 10mg 3r / d; antihypoxants (cytochrome C).
7 vitamin therapy.
8 piracetam - 30-160 mg / kg / day 6-8 weeks
3 student messages
Students' speech with a presentation on the topic: "Dispensary observation of a glaucoma patient"- 15 minutes.
4. Consolidation of the material (compilation of clusters and syncwines, situational tasks) - 15 min.
How to create a cluster
1. Write a keyword or sentence in the middle of a large piece of paper or on a chalkboard.
2. Write down words or sentences that come to mind about the topic.
3. As you have ideas, you write them down.
4. Write down as many ideas as come to your mind.
How to make cinquain
Sinkwine is a "poem" consisting of five lines. In syncwine, a person expresses his attitude to the problem.
The order of writing syncwine:
The first line is one keyword that defines the content of the syncwine.
The second line contains two adjectives that characterize this concept.
The third line - three verbs showing the action of the concept.
The fourth line is a short sentence in which the author expresses his attitude.
The fifth line is one word, usually a noun, through which a person expresses his feelings, associations associated with this concept.
Make a cluster by word:
Glaucoma Congenital glaucoma
Disease
Decreased visual acuity
Limitation of the field of view
Disability
Glaucoma attack
Compose syncwine for a word:
Glaucoma Angle-closure glaucoma
Disease
Decreased visual acuity
Limitation of the field of view
Disability
Glaucoma attack
PROBLEM No. 1.
A 72-year-old patient was being treated in the urological department for urolithiasis. After the injection of atropine, severe pains appeared in the left eye, vision deteriorated sharply. Objectively: the visual acuity of the left eye is 0.01, the eye is dense, but painless on palpation, congestive injection of the vessels of the eyeball, the cornea is cloudy. Make a diagnosis.
Prescribe treatment
Acute attack of primary glaucoma of the left eye
PROBLEM No. 2.
During your night shift at the nurse of the second post, an elderly pensioner, suddenly there was an attack of sharp headaches with irradiation to the left eye, which, according to the patient, she had seen badly lately. There was vomiting, pulse slowed down, blood pressure 180/100 mm Hg, which, however, is not uncommon for the patient. On external examination, you could find a moderate narrowing of the left palpebral fissure, redness of the left eyeball, a cloudy and dilated pupil on the left, which almost does not react to light. The patient distinguishes with this eye only the light from the bulb.
Considering the fact that the patient suffered an acute respiratory illness on her legs a few days before this attack, try to make a presumptive diagnosis.
1. Acute iridocyclitis
2. Hemorrhage into the cavity of the eyeball
3. Acute attack of glaucoma
PROBLEM No. 3.
In the eye department of the interdistrict hospital, a middle-aged woman is being examined, whose left eye has the following: visual acuity of 1.0, field of vision is normal; periodically - pain in the eye, accompanied by "blurred" vision, the appearance of rainbow circles around the light source, an increase in intraocular pressure up to 43-46 mm Hg. These exacerbations are quickly relieved by instilling 1% pilocarpine solution every 2-3 hours in combination with instillations of armin solution - in the morning and in the evening. The second eye is clinically healthy.
How do you decide to proceed in this case?
1. Discharge the patient for outpatient treatment
2. Offer the patient an operation
5. Summing up - 5 minutes .
List of used literature
Main literature
1. Dubovskaya L.A. Eye diseases, M., 1986.
2. Ruban E. D. Eye diseases, M., Phoenix, 2010.
3. Morozov V.I., Yakovlev L.A. Pharmacotherapy of eye diseases. M., Meditsina, 2009.
additional literature
Avetisov E.S. Handbook of ophthalmology, M., 1978.
Broshevsky T.I., Bochkareva A.A. Eye diseases, M., 1983.
Dzhaliashvili O.A., Gorban A.I. First aid for acute diseases and eye injuries, M., 1995.
Zhivkov E., Denev V. Eye symptoms in general diagnostics, M., 2000.
Zolotareva M.M. Eye diseases, M., 1964.
Kapaeva V.G. Eye diseases M .: Medicine 2002.
Kovalevsky E.I. Ophthalmology M .: Medicine 2006.
Kovalevsky E.I. Course Guide to Practical Exerciseseye diseases, M., 2007.
Krasnov M.L., Margalis M.G. Outpatient Ophthalmology,M., 1969.
Ryabchikova T.V., Nazarova N.A. Nursing process of educational method-cheskoe allowance, M., 2000.
E. I. Sidorenko Ophthalmology M .: "GEOTAR - MED" 2003.
Shilyaev V.G. Ophthalmology paramedical workdepartments of hospitals and clinics, M., 1999.
GLAUKOMA - comes from the ancient Greek meaning
green, light blue.
Glaucoma is a serious disease that occurs in all
the world and usually affects people over the age of 40, but
rarely occurs at a younger age.
Glaucoma accounts for about 4% of all eye diseases. How
evidenced by the results of mass preventive
examinations, among a healthy population aged 40 and
older, the disease occurs in 1-2% of cases.
In all countries of the world, glaucoma is one of the first
places as the cause of blindness.
The problem of successfully combating glaucoma blindness is not
only the task of eye doctors, but it is also a general medical
task. Therefore, doctors of all specialties should know
signs of this disease and be able to treat glaucoma.
It is the duty of doctors of all specialties to participate in
carrying out active preventive measures
contributing to early detection of the disease and treatment,
which prevents blindness from glaucoma.
Glaucoma classification
primarysecondary
congenital
Primary glaucoma is one of the most common causes of irreversible blindness. In its development, there are 2 main pathophysiological mechanisms:
intraocular outflow disturbancefluid in the anterior ocular
apples;
optic atrophy
Direction of action of intraocular pressure
Open-angle glaucoma (OAG)
The pathogenesis of open-angle glaucoma is associated with a violationthe function of the drainage system of the eye, through which
outflow of fluid from the eye. With histological examination
eyes with OAG in the drainage zone of the limbus are always found
dystrophic changes. In the initial stage of the disease
trabecular plates thicken, narrow
intratabecular fissures and especially the scleral sinus. V
further, the trabecula is completely reborn, the cracks in it
disappear, the scleral sinus is overgrown. Recently
data has accumulated that indicate an important role in
pathogenesis of OAG of the functional block of the Schlemm canal. Everything
these changes to a certain extent depend on the nervous,
endocrine and vascular disorders, therefore primary
glaucoma is combined with diseases such as
atherosclerosis, hypertension, diabetes, damage
submontane area.
Both the anatomical features of the glaucomatous eye and
the nature and degree of dystrophic changes in the drainage
apparatus are determined by genetic factors, due to
than, primary open-angle glaucoma is often
hereditary character. Very often, OAG occurs and progresses imperceptibly for
a sick person who does not experience any unpleasant
sensations and consults a doctor when noticing significant
deterioration of vision. Usually normal due to some stagnation in
veins of the head due to the horizontal position of the body in
sleep time (in the morning) IOP is slightly increased, and by the end of the day it
decreases slightly. The amplitude of fluctuations P is not normal
exceeds 5 mm Hg In glaucoma, these fluctuations
much bigger. The first and leading sign in
glaucoma is the presence of ophthalmotonus more than 27 mm Hg.
Art., and fluctuations in the flow of the grids over 5 mm Hg. At
the transition from the initial stage to the developed stage is marked by the second
a sign of glaucoma is a change in visual function,
consisting in narrowing the field of view and decreasing acuity
vision. Usually, the narrowing of the visual field begins with the nasal
sides. The third cardinal sign of glaucoma is
expansion of the exudation of the optic nerve head, develops
in its later stages, due to expansion and protrusion
posteriorly, under the influence of increased IOP, lattice plate
and atrophy of nerve fibers and glial tissue. Fourth
sign - retinal edema, which is determined by
an increase in the size of the blind spot.
Pseudoexfoliative glaucoma
Angle-closure glaucoma (ZUG)
The main link in the pathogenesis of ZUG is blockadeangle of the anterior chamber by the root of the iris,
which arises as a result of functional
block of the pupil.
Functional or relative pupillary
blockage occurs in eyes with overly anterior
the location of the lens.
In such eyes, the iris is tightly attached to the anterior
the surface of the lens, making it difficult for outflow
liquid from the rear chamber to the anterior chamber. it
leads to increased pressure in the rear chamber
eyes and protrusion of the iris anteriorly,
as a result, the angle of the anterior chamber
narrows, and under certain conditions the angle
closes. A definite role in the pathogenesis of ZUH
belongs to genetic, nervous, endocrine
and vascular factors. Angle-closure glaucoma is common
(about 90% of all cases). This variety
glaucoma usually begins with an acute or
subacute attack.
Diagnosis of ZUH during acute and subacute
it is not difficult to deliver an attack. For early
diagnostics of ZUG use load
samples, of which the most effective and
safe dark and positional (face down).
The patient is placed for 1 hour in a dark room,
the sample is considered positive if
ophthalmotonus during this period will not increase
less than 5 mm Hg, and positional test
lies in the fact that the patient is laid
on the couch, face down, also for 1 hour.
Increase in ophthalmotonus by 5 mm Hg. Art. and
more indicates a predisposition to
blockade of the anterior chamber angle. the effect
dark test is associated with pupil dilation in
darkness, positional test - with displacement
lens under the influence of gravity to the side
cornea.
Intraocular fluid flow in angle-closure glaucoma
Acute attack of glaucoma
Acute attack - occurs under the influence of various factors, withemotional stress, with prolonged stay in the dark, with
drug-induced dilation of the pupil or for no apparent reason.
The patient complains of pain in the eye and head, blurred vision,
the appearance of rainbow circles when looking at a light source. Painful
sensations are associated with squeezing the nerve elements of the rainbow root
shell and ciliary body.
With a pronounced attack, nausea and vomiting may occur.
The pains radiate to individual organs - the heart, the abdomen, which
sometimes causes diagnostic errors. With an objective
examination conspicuous stagnant injection of the vessels of the eye
apples. Cornea edematous, like misted glass, anterior chamber
small (slit) pupil is dilated.
The expansion of the pupil is associated with paresis of its sphincter, caused by a sharp
increased IOP. The iris is edematous, posterior synechiae are formed. Ocular fundus
seen in the fog:
the optic disc is edematous, with indistinct contours. Often
you can see the pulsation of the retinal artery and sometimes hemorrhages on the disc and
beside him.
During an acute attack, IOP rises to 70 mm Hg, outflow
fluid from the eye stops completely.
Gonioscopy reveals complete closure of the anterior chamber angle.
A subacute attack of glaucoma is characterized by the same basic
symptoms, however, they are much less pronounced.
Accumulation of fluid behind the vitreous body in malignant glaucoma - ciliary block
Differential diagnosis of an acute attack of glaucoma and acute iritis (iridocyclitis).
Acute glaucoma attack Acute iritisaccompanied by complaints
(iridocyclitis). Raduzhnykh
on rainbow circles at
no circles. Prevail
looking at the light.
pain in the eye. Eye
Prevail
falls ill suddenly.
radiating pain.
Prevails
Often preceded by
pericorneal
prodromal seizures.
injection. Cornea
Stagnant injection
transparent.
vessels. Cornea
Sensitivity
diffusely cloudy.
the cornea is preserved.
Sensitivity
Anterior chamber depth
the cornea is missing.
normal or
The anterior chamber is shallow.
uneven. Iris
The iris color is not changed,
hyperemic, changed
or changed
in color, the relief is smoothed.
insignificantly. Pupil
The pupil is constricted. IOP is normal
wide, IOP sharply
or downgraded.
increased.
Classification of primary glaucoma
The formStage
State
IOP
Dynamics
visual
functions
Closed-angle
Open angle
Mixed
Initial (I)
Developed (II)
Far
visiting
(III)
Terminal (IV)
Normal
(A) T≤26mm Hg
Moderately
increased
(B) T = 26-32 mm
Stabilized
Unstabilized
hg
High (C)
T≥33 mm Hg
Acute attack of angle-closure glaucoma
Additional classification scheme for primary glaucoma
The formClosed-angle
Variety
With pupillary block
Creeping
Flat iris
With vitreo lens
block (malignant)
Place of the main part
outflow resistance
Pretrabecular
the cloth
Open Angle Simple
Pseudoexfoliative
Pigment
Trabecular tissue
Intrascleral zone
(including collapse
Schlemm's Canal)
Mixed
Combined
defeat
Clinical signs of the disease
In the diagnosis of the form of glaucoma, in addition to the clinical picture, gonioscopy is of great importance - a method of examining the angle of the anterior chamber
This requires the presenceslit lamp and goniolines.
Goldman's three-mirror lens. It is used for gonioscopy - the study of the angle of the anterior chamber.
The degree of opening of the anterior chamber angle (Grade 0 - corner closed, Grade 4 - corner open)
The degree of opening of the anterior chamber angle according to Schaffer
Gonioscopic picture in open-angle glaucoma
Gonioscopic picture of the anterior chamber angle in angle-closure glaucoma
Scheme of a gonioscopic picture in pigmentary glaucoma
Gonioscopic picture in pigmentary glaucoma
Anterior chamber angle in congenital glaucoma
Phakolytic glaucoma
I. Initial stage. At this stage, the primaryglaucoma is not noted marginal excavation
Optic nerve disc and pronounced changes in the field of vision.
Expansion may be observed
physiological excavation of the optic nerve disc, the appearance
small livestock in the field of view (scotoma
Bjerrum - rice A) and increase in size
blind spot.
II. Developed stage. For this stage
characteristic persistent narrowing of the field of view by 100
from the nasal side and its concentric
narrowing. There is an edge excavation of the optic nerve disc.
III. A far-advanced stage. This stage
characterized by persistent narrowing of the field
vision from the nasal side or concentrically
up to 150 from the gaze fixation point.
IV. The diagnosis "Terminal glaucoma" can
be installed in complete absence
vision (Visus = 0) or the presence of light perception with
improper light projection (1 / ∞ l. incertae)
with at least partial transparency
wednesday
Automatic perimetry
This is how patients with glaucoma see
Developed stage (II)Far-reaching stage (III) The optic nerve is normal
Glaucomatous
excavation The optic nerve is normal
Glaucomatous
excavation
Physiological excavation of the optic nerve head
Expansion of physiological excavation at the initial stage of glaucoma.
Marginal glaucomatous excavation with advanced stage of glaucoma
Tonometry - an objective method for measuring intraocular pressure
To assess intraocularpressure (IOP) is more often used 10g
Maklakov's tonometer and taken
the following gradations: A -
normal pressure (16 - 26 mm
Hg); B - moderately increased
(27-32 mm Hg); C - high (33 and
above mmHg)
Congenital glaucoma
Congenitalglaucoma
Congenital iridocorneoendothelial syndrome
Classification of secondary glaucoma
1. Inflammatory andpost-inflammatory glaucoma:
a) caused by sclerites and
keratitis;
b) postuveal;
c) with heterochromic uveopathy.
2. Phakogenic glaucoma:
a) phakotopic;
b) phakomorphic;
c) phakolytic.
3. Vascular glaucoma:
a) neovascular;
b) phlebohypertensive.
4. Dystrophic glaucoma:
a) with retinal detachment;
b) with iridocorneal
endothelial syndrome;
c) with primary systemic
amyloidosis;
d) hemolytic.
5. Traumatic glaucoma:
a) contusion;
b) wound;
c) burn;
d) radiation.
6. Postoperative glaucoma:
a) aphakic;
b) after keratoplasty;
c) after surgery for detachment
retina.
7. Neoplastic glaucoma:
a) with intraocular tumors;
b) with tumors of the orbit and
endocrine exophthalmos.
Rubeosis of the iris. Secondary neovascular glaucoma
Phakolytic glaucoma
Conservative treatment
To reduce IOP, miotics are widely used, which are divided intocholinomimetic and anticholinesterase. Under the influence of miotics, rainbow
the shell is pulled away from the angle of the anterior chamber, its rigidity increases and
bombing decreases. This mechanism is important in the ZUG. From
cholinomimetics use a solution of pilocarpine hydrochloride 1%, 2%, 4%,
carbacholine 0.75% - 3%. The disadvantage of cholinomimetics is the short duration
their actions (4-6 hours).
In clinical practice, the following miotics of anticholinesterosis are used
actions: phosphacol 0.02%, armin 0.05%, 0.01%, fosarbine 0.01%, pibufin 0.025%,
tosmilen 0.1-1%.
All of these drugs are stronger than cholinomimetics. Their miotic action
lasts more than a day. Long-term use of anticholensterotic miotics
action often causes the development of cataracts.
Sympathicotropic drugs. From this group of drugs for the treatment of glaucoma
use epinephrine, fetanol and euspiran. The mechanism of hypotensive action is associated
with an improvement in the outflow of fluid from the eye and to a decrease in the formation of watery
moisture. A good effect is given by adrenopilocarpine. In recent years, widespread use
received β-blockers. These drugs lower IOP by suppressing production
aqueous humor. Timolol 0.25% or 0.5% 1-2 times a day.
Carbonic anhydrase inhibitors - these drugs reduce the rate of formation
watery moisture by 50%. The most widespread is acetazolamide under
the name "diacarb". It is prescribed orally 0.125-0.5 g 1-2 times a day (most often
O, 25g is applied 2-4 times).
Osmotic agents: urea 10% solution, IV mannitol 20% solution, ascorbate
sodium i.v. 20% solution, Glycerol inside.
TREATMENT OF ACUTE AND SUB-ACUTE ATTACK OF GLAUCOMA
Instillations of 1-2% are prescribed within 1 hourpilocarpine into the conjunctival sac every 15 minutes,
then every 1/2 hour, and then every hour (2-3 times).
After 6 hours, the frequency of instillation is reduced to 6 times per
day. Timolol is prescribed simultaneously with miotics.
or clonidine (2-3 times a day), oral diacarb (0.5 g,
then 0.25 g 4 times a day), glycerin (1-2 times a day), i.m.
lasix, 2h. hot foot baths. Useful 2-3 leeches for
temple, after 3-4 hours i / m chlorpromazine or lytic mixture
(chlorpromazine, diphenhydramine, promedol). If in a day
the attack does not stop, the operation of iridoectomy is indicated.
Intraocular fluid flow after iridectomy
Laser trabeculoplasty. Effective in the early stages of open-angle glaucoma. A painless procedure and is performed on an outpatient basis
conditions.Iridectomy is a fistulizing operation that is effective for angle-closure glaucoma
Surgical iridectomyLaser iridectomy
Sclerectomy is a fistulizing operation in which an additional pathway is created for the outflow of intraocular fluid into the intrascleral veins
Sclerectomy is a fistulizing operation in whichan additional pathway for intraocular outflow is created
fluid into intrascleral veins. Effective for many
types of glaucoma and has many modifications. Glaucoma
CCax
Nuri Kumari
Chaudhary Suman
Lamichkhane Sharmila
ml-402
GLAUCOMA
Glaucoma
Completed
Chaudhary Suman
Sah Nuri Kumari
Lamichkhane Sharmila
ML-402 DEFINITION
Glaucoma-
this is
disease
eye,
characterized, characterized by: constant
or periodic increase in intraocular
pressure, characteristic changes in the field of vision,
decline
sharpness
central
vision,
by excavation of the optic nerve and ending
blindness in the absence of rational treatment
:
3% of patients
APPLY TO
RECEPTION
20% OF THE BLIND LOSE
VISION CONSEQUENCE
GLAUCOMS The character for them is
disturbances in the circulation of aqueous humor
(BB), leading to a deterioration of its outflow from
eyes;
IOP is higher than the visual tolerance
nerve level;
ischemia and hypoxia of HHN;
glaucoma optic neuropathy;
degeneration (apoptosis) of ganglion cells
retina. Intraocular pressure
1.It maintains a spherical shape
eyeball and correct topographic
the relationship of its internal structures,
2. Facilitates metabolic processes in these structures
3.It has an effect on circulation
blood in the intraocular vessels
* IOP level is relatively stable and variable
only in case of impaired circulation of explosives. Circulation of aqueous humor
Moisture fills the posterior and anterior chambers of the eye and
flows mainly into episcleral veins along the drainage
the eye system located on the anterior wall of the corner
anterior chamber.
BB first enters the posterior chamber of the eye and then through
the pupil passes into the anterior chamber, which serves as its
the main reservoir.
With close contact of the iris with the lens, the transition
fluid from the rear chamber to the anterior chamber is difficult that
leads to increased pressure in the rear chamber Circulation of aqueous humor Anterior chamber angle (UPK) -
the narrowest part of the anterior chamber.
The front wall of the UPK is formed by a ring
Schwalbe, TA and scleral spur, posterior -
the root of the iris, the apex is the base
ciliary crown Wide angle (40-45 °) -
all structures of the CCP (IV) are visible,
medium narrow (25-35 °) - determined
only part of the top of the corner (W),
narrow (15-20th) - ciliary body and scle
the spur is not visible (II),
visible slit (5-10 °) - determined only
part of TA (I),
closed - the structures of the Criminal Procedure Code are not
viewed (0).
Anterior chamber angle classification
eyes in width, a - wide; b -
medium width; в - narrow; G -
slit Drainage system
1.Trabecular apparatus - annular porous
crossbar between the front and rear edges
internal scleral groove
2.Schlemmian canal - scleral sinus located in
posterolateral part of the internal scleral groove
3. Outflow from the Schlemmov canal through 20-30 collector
canals in veins episclera GLAUK CLASSIFICATION
1.
2.
3.
4.
I. Primary
According to the state of the anterior chamber angle
Open angle
- Closed-angle
Mixed
By stages of development
- Initial
- Developed
- Far-gone
- Terminal
As of vgd
- NORMAL (UP TO 27 mm)
- MODERATE INCREASED (28-32 mm)
- HIGH (OVER 32 mm)
By the dynamics of visual functions
- Stabilized
- Unstabilized
II. Secondary
III. Congenital
IV. Juvenile closed charcoal glaucoma (ZUG), with
which an increase in IOP is caused by a block
CPC by intraocular structures
(iris, lens, glass like
body) or goniosinechia,
open-angle glaucoma (OAG),
caused by damage to the drainage
eye systems,
mixed glaucoma, in which
both mechanisms of IOP increase are combined. Primary angle-closure glaucoma
Anatomical prerequisites -
1.small size of the eyeball;
large lens size;
anterior attachment of the iris to the CG
2.Aging changes - flattening
cornea, atrophy of the iris in the root area. The pathogenesis of PZUG is the closure of the UPC by the root of the iris.
The following mechanisms of such a blockade are described.
As a result of the tight fit of the edge of the pupil to
the lens, BB accumulates in the posterior chamber of the eye, which
leads to protrusion anteriorly of the root of the iris and
blockade of the Criminal Procedure Code (Fig. 17.21).
Basal fold of the iris, formed when
dilation of the pupil, closes the filtration zone
narrow UPK in the absence of pupillary block.
Displacement of the vitreous humor anteriorly as a result
accumulation of fluid in the posterior segment of the eye can
lead to the emergence of vitreous lens block.
In this case, the root of the iris is pressed by the lens to
the front wall of the UPK
As a result of the formation of adhesions (goniosinechia) and
adhesion of the root
iris with the anterior wall of the CPC occurs
obliteration. Closed-angle glaucoma
1.Proceeds paroxysmal, eye hurts
2.Reduced horny sensitivity
shell
3 edema of the cornea
4 stagnant injection
5.Small front camera
6.The corner of the anterior chamber is closed by the root
irises
7 rainbow circle complaints
8.High intraocular pressure (eye
dense as a stone)
9 dilated pupil Acute Glaucoma Attack
A state of sharp and significant increase
intraocular pressure above 50 mm Hg
Development mechanism
1.Disruption of fluid circulation
2. Accumulation of excess liquid CLINIC
1 blurred vision
2 the appearance of rainbows
circles around the source
Sveta
3.Sharp pain in the eye
4.bombing the iris
5.Reduced pungency
vision
6 nausea
7 vomiting
8 dizziness Diagnosis of the disease
Superficial examination of the eye
redder eyes
dilated oval pupil
lack of reaction to light)
1.
2. On palpation
increased tone
soreness An acute attack of glaucoma requires
emergency medical care
1. Miotics: pilocarpine 1-4% every 15 minutes for
1 hour, every hour during the day
2.ß - blockers 3 times a day
3. Diuretics:
diacarb 0.25 - 4 times a day or IV
4.furosemide 40 mg
5. Distracting procedures:
leeches on the temple, mountains. Foot
baths
If the attack does not stop - after 12 - 24 hours
surgical treatment Open angle glaucoma
Anatomical prerequisites -
1.weak scleral development
spurs and ciliary muscle,
posterior attachment to the sclera;
large lens size;
anterior attachment of the iris to
CT
2.Age-related changes in the trabecular
apparatus, ciliary body, atrophy
irises
3. Genetic predisposition The pathogenesis of POAG includes three main
pathophysiological mechanism:
hydromechanical,
hemocirculatory and
metabolic.
The first one starts with
deterioration of IV outflow from the eye and
increase in IOP.
Outflow deterioration caused by
trabeculopathy - dystrophic
changes in TA. 2.Increased IOP causes
decreased perfusion blood
pressure and intensity inside
ocular circulation, as well
deformation of two mechanically weak
structures - trabecular diaphragm in
drainage system of the eye and trellis
scleral plates.
3.Hemocirculatory disorders can
divided into primary and secondary.
Primary violations precede
increase in IOP, secondary occur in
as a result of the action of increased IOP on
hemodynamics of the eye.
Clinic.
1. Complaints are absent or mild
2. Biomicroscopy: symptoms of "cobra" and "emissary"
3. Destruction of the pigment border
4.Pseudoexfoliation
5.Depigmentation of the iris
6. Intraocular pressure is increased (not always)
7 progressive narrowing of the visual field
8.Excavation of the optic nerve head
9.Open angle of the anterior chamber
10 Decreased central vision Primary open-angle glaucoma.
Gonioscopy.
1.Sclerosis of trabeculae
2. Pseudo-exfoliation in the CPC
3. Deposition of pigment granules in
CPC DIAGNOSTICS
1.
2.
3.
4.
5.
1.
1.
2.
1.
2.
I. Complaints
Feeling of pressure in the eyes
Feeling of "tears", foreign body
"Black flies" before the eyes
Photopsy
Earlier presbyopia
II. Determination of IOP
Maklakov tonometry and daily tonometry
III. Study of the angle of the anterior chamber
Gonioscopy
Wurgaft method
3.Subjective assessment of the optic disc condition
IV. Research of peripheral vision
Perimetry
Campimetry
V. Biomicroscopy and ophthalmoscopy Increased IOP
1 Blockade of RRU (corneal iris
angle) by the root of the iris
2 Parietal blockade of RRU alien
cloth
3 Defeat of the outflow tract in
indoor or outdoor
walls of the Schlemm canal
4 BB hypersecretion
IOP assessment in glaucoma
A - normal
20 - 26 mm Hg Art.
B - moderately increased to
32 mmHg Art.
C - high 33 mm Hg. Art. and TONOMETRY ACCORDING TO MAKLAKOV Perimetry
NORM Early visual field changes
Extension of the blind
stains
2.Scotomy in the zone
Bjerrum (from 10 to
20 °)
3.Scotome Seidel -
arcuate
scotoma in the zone
Bjerrum
4. Rene's step
1.
Late changes
field of view
1.Ring-shaped
or double
arcuate
scotoma
2. Narrowing
nasal halves
3. Residual
central and
temporal
islets Late field changes
vision Excavation optic nerve disc PROGRESSIVE LOSS OF VISUAL FIELDS IN GLAUCOM.
Target -
1.Reduce IOP by 30%
2.Affect microcirculation
in vessels
3. Improve nutritional status of MN and
retina (neuroprotective agents,
antioxidants) Medication for glaucoma
1.Preparations affecting the outflow of high fluid
2.Preparations that reduce production
VGZH
3.Combined preparations The mechanism of their influence on IOP is associated with or
with improved outflow of explosives from the eye
1.Miotics
2.Adrenaline
3.latanoprost
decreased secretion of intraocular
liquids
1.a2-adrenoagonists,
2.r-adrenergic blockers,
3. carbonic anhydrase inhibitors. Of the cholinomimetics used to reduce IOP
1.1% Pilocarpine hydrochloride
2.Pilocarpine hydrochloride
1% solution with methylcellulose
3. Carbocholine
4. Aceclin is used in the form of eye drops 3-6 times a day. Miotics cause contraction of the sphincter of the pupil
and ciliary muscle,
promote the expansion of blood vessels and
increasing their permeability.
Narrowing the pupil and pulling the fold of the iris away from
UPC, miotics improve the access of the IV to the drainage
the eye system.
At the same time, due to contraction of the ciliary
the muscles are stretched trabecular diaphragm,
the blockade of the Schlemm canal is reduced and
the outflow of explosives from the eye improves. Latanoprost (Xalatan) - eye drops 0.005%
concentration - represents
synthetic analogue of prostaglandin F2o.
Latanoprost has a pronounced and
prolonged hypotensive effect,
which is explained by the improvement of uveoscleral
outflow B B from the eye.
The drug is used once a day. adrenostimulants in clinical practice
use
epinephrine dipivalate (dipivefrin) and
a2 - adrenoagonist (clonidine, clonidine). Carbonic anhydrase inhibitors
Acetazolamide
Dorzolamide hydrochloride Glaucoma laser surgery. Laser
surgery is aimed primarily at
elimination of intraocular blocks on the way
BB movements from the posterior chamber of the eye to
episcleral veins. Laser iridetomy
consists in the formation of a small hole in
peripheral iris.
The operation is indicated for functional or organic
block of the pupil.
It leads to equalization of pressure in the rear and front
chambers of the eye and the opening of the Criminal Procedure Code. For preventive purposes
the operation is performed in all cases of closed-angle glaucoma
and with an open-angle glau coma with a narrow UPK.
.Laser trabeculopasty consists of
applying a series of moxibustion on the inner
surface of the trabecular diaphragm, in
as a result, its permeability for
BB and
the danger of a blockade of the Schlemm canal is reduced.
The indication for surgery is POAG, not
compensable by
medicines Glaucoma microsurgery.
Micro surgical operations are performed using
operating microscope and special microinstruments
cops
There is a wide variety of operational
interventions that can be divided into 4 main
groups ..
Iridectomy
Fistulizing operations
trabeculectomy
Cyclodestructive operations Operations that improve the circulation of explosives inside
eyes, - iridectomy
(elimination of pupillary block) and
iridocycloretraction (expansion of the CPC).
The indication for these operations is
primary or secondary angle-closure glaucoma.
Fistulizing operations allow
create a new pathway for the outflow of explosives from the anterior chamber to
subconjunctival space, whence the liquid
bone is absorbed into the surrounding vessels.
(trabeculectomy) Non-Penetrating Filtering Operations (NFO) based
on subscleral excision of the outer wall of the scleral
sinus (sinusotomy) in combination with trabecu stretching
lary wall using micro moxibustion
According to one of the modifications of the operation (non-perforating
deep sclerectomy) deep limbo plate
scleral tissue is excised not only over Schlemm's
canal, but also anteriorly to Descemet's sheath.
The effectiveness of NPO increases with the use of anti
metabolites during or after surgery. Decrease
the severity of the antihypertensive effect of NPO in
the postoperative period is an indication for
laser perforation of the trabecular diaphragm in the area
operations Cyclodestructive operations are based on
damage and subsequent atrophy of part of the processes
ciliary muscle, which leads to
a decrease in explosive production. Of the modifications of this
operations are the most widespread
cyclo-cryodestruction.
In the process of performing the operation, several
cryoapplications on the sclera in the area of location
ciliary crown.
With sufficient intensity and for a long time
cryotherapy can achieve significant
decrease in IOP.
The length of the impact zone should not exceed
180-200 ° to exclude hypotension and atrophy transscleral diode laser
cyclocoagulation,
characterized by greater safety and high
efficiency.
Cyclodestructive operations are shown at far
advanced glaucoma, as an additional
unsuccessful or incomplete intervention
effect of previously produced fistulas
operations and for terminal glaucoma with painful syncope
drome.
What is the Android status bar?
How to choose a gift for the new year for yourself
How to choose gifts for the New Year?
Excel status bar options What the status bar is for
Complete Lessons - Knowledge Hypermarket