heart blood supply innervation lymph drainage
The heart (Latin cor, Greek cardia) is a hollow fibromuscular organ that, functioning as a pump, ensures the movement of blood in the circulatory system.
The heart is located in the anterior mediastinum in the pericardium between the leaves of the mediastinal pleura. It has the shape of an irregular cone with a base at the top and a top facing downward, to the left and anteriorly. The size of the heart is individually different. The length of the heart of an adult varies from 10 to 15 cm (usually 12-13 cm), the width at the base is 8-11 cm (usually 9-10 cm) and the anteroposterior size is 6-8.5 cm (usually 6, 5 --7 cm). The average heart weight in men is 332 g (from 274 to 385 g), in women - 253 g (from 203 to 302 g).
In relation to the midline of the body, the heart is located asymmetrically - about 2/3 to the left of it and about 1/3 to the right. Depending on the direction of the projection of the longitudinal axis (from the middle of its base to the apex) on the anterior chest wall, a transverse, oblique and vertical position of the heart is distinguished. The upright position is more common in people with a narrow and long chest, transverse - in people with a wide and short chest.
The heart consists of four chambers: two (right and left) atria and two (right and left) ventricles. The atria are located at the base of the heart. The aorta and the pulmonary trunk emerge from the heart in front, the superior vena cava flows into it in the right part, the inferior vena cava flows into the posterior inferior, the left pulmonary veins are located behind and on the left, and the right pulmonary veins are somewhat to the right. Distinguish between the anterior (sternocostal), lower (diaphragmatic), which in the clinic is sometimes called the posterior, and the left lateral (pulmonary) surface of the heart. The right edge of the heart is also distinguished, formed mainly by the right atrium and adjacent to the right lung. The anterior surface, adjacent to the sternum and cartilage of the left III-V ribs, is represented over a greater extent by the right ventricle, on a lesser extent - by the left ventricle and atria. The border between the ventricles corresponds to the anterior interventricular groove, and between the ventricles and the atria - the coronary groove. In the anterior interventricular sulcus, the anterior interventricular branch of the left coronary artery, the great vein of the heart, the nerve plexus and the diverting lymphatic vessels are located; in the coronary sulcus, the right coronary artery, nerve plexus and lymphatic vessels. The diaphragmatic surface of the heart faces downward and is adjacent to the diaphragm. It is composed of the left ventricle, partly the right ventricle, and sections of the right and left atria. On the diaphragmatic surface, both ventricles border each other along the posterior interventricular groove, in which the posterior interventricular branch of the right coronary artery, the middle vein of the heart, nerves and lymphatic vessels pass. The posterior interventricular groove near the apex of the heart connects to the anterior one, forming a notch of the apex of the heart. The silhouette of the frontal projection of the heart onto the anterior chest wall has right, lower and left borders. The right border is formed at the top (II - III rib) by the edge of the superior vena cava, below (III - V rib) - by the edge of the right atrium. At the level of the V rib, the right border passes into the lower one, which is formed by the edge of the right and partially left ventricles and goes obliquely down and to the left, crossing the sternum above the base of the xiphoid process, to the intercostal space on the left and further, crossing the cartilage of the VI rib, reaches the V intercostal space by 1 , 5 cm medially from the midclavicular line. The left border is formed by the aortic arch, pulmonary trunk, left ear of the heart and left ventricle. The exit sites of the aorta and the pulmonary trunk are projected at the level of the III intercostal space: the aortic mouth is behind the left half of the sternum, and the pulmonary trunk mouth is at its left edge.
The structure of the chambers of the heart corresponds to its function as a pump. The right atrium with the right ventricle, the left one with the left, communicates, respectively, through the right and left atrioventricular openings, equipped with valves that ensure the direction of blood flow from the atria to the ventricles during their diastole and prevent backflow during ventricular systole. The communication of the cavities of the ventricles with the arteries is regulated by valves located in the orifices of the aorta and the pulmonary trunk. The right atrio-gastric valve is called tricuspid (tricuspid), the left - bicuspid, or mitral.
The right atrium has an irregular cubic shape; its capacity in an adult ranges from 100-140 ml, the wall thickness is 2-3 mm. On the right, the atrium forms a hollow process - the right ear. Its inner surface has a number of ridges formed by bundles of comb muscles. On the lateral wall of the atrium, the comb muscles end, forming an elevation - the border ridge (crista terminalis), which on the outer surface corresponds to the border groove (sulcus terminalis). The medial wall of the atrium - the interatrial septum - has an oval fossa in the center, the bottom of which is formed, as a rule, by two sheets of the endocardium. The height of the fossa is 18-22 mm, the width is 17-21 mm.
The shape of the right ventricle approaches a trihedral pyramid (base facing upwards), the medial wall of which belongs to the interventricular septum. The capacity of the right ventricle in adults is 150-240 ml, the wall thickness is 5-7 mm. The weight of the right ventricle is 64-74 g. In the right ventricle, two parts are distinguished: the ventricle itself and the arterial cone, located in the upper left part of the ventricle and continuing into the pulmonary trunk. The diameter of the opening of the pulmonary trunk is 17-21 mm. Its valve consists of 3 semi-moon flaps: front, right and left. In the middle of each semilunar flap, there are thickenings (nodules) that contribute to a more hermetic closing of the flaps. The inner surface of the ventricle is uneven due to fleshy trabeculae extending in different directions, which are poorly expressed on the interventricular septum. The right atrioventricular (atrioventricular) opening, located at the top of the ventricle (to the right and behind the opening of the pulmonary trunk), has an oval shape; its longitudinal size is 29-48 mm, transverse - 21-46 mm. The valve of this opening, like the mitral valve, consists of an annulus fibrosus; the valves, which are attached with their base to the fibrous ring (the free edges of the valves face the cavity of the ventricle); tendinous chords running from the free edges of the valves to the wall of the ventricle, to the papillary muscles or fleshy trabeculae; papillary muscles formed by the inner layer of the ventricular myocardium. The number of valve cusps only slightly more often than in half of the cases corresponds to its designation "tricuspid"; it ranges from 2 to 6, with a greater number of valves found with large sizes of the atrioventricular opening. At the point of attachment, anterior, posterior and septal valves and the corresponding papillary muscles are distinguished, with the tops of which the valves are connected by tendon chords. A large number of papillary muscles occurs with an increased number of valves.
The left atrium, which is close to a cylindrical shape, forms an outgrowth on the left - the left ear. The capacity of the left atrium is 90-135 ml, wall thickness is 2-3 mm. The inner surface of the atrial walls is smooth, except for the walls of the ear, where there are ridges of the comb muscles. On the back wall are the mouths of the pulmonary veins (two on the right and two on the left). On the interatrial septum from the side of the left atrium, the valve of the oval opening (valvula foraminis ovalis) fused with the septum is noticeable. The left ear is narrower and longer than the right one; it is delimited from the atrium by a well-defined intercept.
The left ventricle is tapered. Its capacity is from 130 to 220 ml, wall thickness is 11-14 mm. The mass of the left ventricle is 130-150 g. Because of the roundness of the left edge of S., the anterior and posterior walls of the left ventricle are not sharply demarcated, the medial wall corresponds to the interventricular septum. The area of the left ventricle closest to the aortic opening is called the arterial cone. The inner surface of the ventricle, with the exception of the septum, has numerous fleshy trabeculae. There are two openings at the top: on the left and in front - the oval left atrioventricular (its longitudinal size is 23-37 mm, transverse - 17-33 mm), on the right and back - the opening of the aorta. The valve of the left atrioventricular opening (mitral) most often has two cusps and, accordingly, two papillary muscles - anterior and posterior. The aortic valve is formed by three semilunar valves - posterior, right and left. The initial part of the aorta at the location of the valve is expanded (its diameter reaches 22-30 mm) and has three depressions - the sinuses of the aorta.
The walls of the heart are formed by three membranes: the outer one is the epicardium, the inner one is the endocardium and the muscular membrane located between them is the myocardium. The epicardium - the visceral plate of the pericardium - is the serous membrane. It consists of a thin plate of connective tissue with a different arrangement of elastic and collagen fibers, covered from the surface with mesothelium. The myocardium (Fig. 5) makes up the bulk of the heart wall. The ventricular myocardium is separated from the atrial myocardium by fibrous rings, from which the bundles of myocardial fibers begin. In the myocardium of the ventricles, it is conditionally possible to distinguish the outer, middle and inner (deep) layers. The outer layers of the ventricular myocardium are common. The course of the fibers of the outer and inner layers has the form of a rare spiral; the middle layer of the bundles of the myocardium is circular. Histologically, myocardial tissue differs from striated skeletal muscle tissue in a number of features, incl. the smaller size of myocardial cells (cardiomyocytes) and sarcomeres, the presence of one nucleus in the cell, connecting the cardiomyocytes in series with each other end-to-end by means of insertion disks, etc. About 30-40% of the volume of the cardiomyocyte is occupied by mitochondria. The special saturation of cardiomyocytes with mitochondria reflects the high metabolic rate of tissue with continuous activity. In the myocardium there is a special system of fibers that have the ability to conduct impulses to all muscle layers of C. and coordinate the sequence of contraction of the wall of the chambers of C. These specialized muscle fibers constitute the conducting system of the heart. It consists of the sinus-atrial and atrioventricular nodes and bundles (atrial, internodal connective, atrioventricular and its branches, etc.). In the tissue of the S.'s conducting system, which is more adapted to anaerobic metabolism than the contractile myocardium, mitochondria occupy about 10% of the cell volume, and myofibrils - about 20%. The endocardium lines the S. cavity, including the papillary muscles, tendon chords, trabeculae and valves. In the ventricles, the endocardium is thinner than in the atria. It, like the epicardium, consists of two layers: subendothelial and collagen-elastic, covered with endothelium. The leaflet of the heart valve is a fold of the endocardium, in which there is a connective tissue layer.
The ratio of the heart and its parts to the anterior chest wall changes depending on the position of the body and breathing movements. So, when the body is on the left side or in an anteriorly inclined state, the heart is closer to the chest wall than in opposite body positions; when inhaling, it is farther from the chest wall than when exhaling. In addition, the position of the heart changes depending on the phases of cardiac activity, age, gender and individual characteristics. The heart lies behind the lower half of the sternum, and the large vessels lie behind the upper half. The left venous opening (bicuspid valve) lies to the left of the sternum in the third intercostal space; the work of the valve is heard at the apex of the heart. The right venous opening (tricuspid valve) is projected behind the sternum on a line drawn from the cartilage of the III rib on the left to the cartilage of the V rib on the right; the work of the valve is heard at the edge of the sternum in the fourth intercostal space on the right.
The heart is located asymmetrically in the anterior mediastinum. Most of it is to the left of the midline, only the right atrium and both vena cava remain on the right. The long axis of the heart is located obliquely from top to bottom, from right to left, from back to front, forming an angle of approximately 40 degrees with the axis of the whole body. At the same time, the heart is, as it were, turned in such a way that its right venous section lies more anteriorly, and the left arterial section lies more posteriorly.
The heart, together with the pericardium, in most of its front surface (facies sternocostalis) is covered by the lungs, the front edges of which, together with the corresponding parts of both pleura, going in front of the heart, separate it from the anterior chest wall, with the exception of one place where the anterior surface of the heart is adjacent through the pericardium to the sternum and cartilage of the V and VI ribs. The boundaries of the heart are projected onto the chest wall as follows. The apex thrust can be felt 1 cm medially from the linea mamillaris sinistra in the fifth left intercostal space. The upper border of the cardiac projection is at the level of the upper edge of the third costal cartilage. The right border of the heart runs 2 - 3 cm to the right from the right edge of the sternum, from the III to the V rib; the lower border runs transversely from the V right costal cartilage to the apex of the heart, the left - from the cartilage of the III rib to the apex of the heart.
The ventricular outlets (aorta and pulmonary trunk) lie at level III of the left costal cartilage; the pulmonary trunk (ostium trunci pulmonalis) - at the sternal end of this cartilage, the aorta (ostium aortae) - behind the sternum somewhat to the right. Both ostia atrioventricularia are projected on a straight line running along the sternum from the third left to the fifth right intercostal space.
With auscultation of the heart (listening to valve sounds with a phonendoscope), the sounds of the heart valves are heard in certain places: mitral - at the apex of the heart; tricuspid - on the sternum on the right against the costal cartilage; the tone of the aortic valves - at the edge of the sternum in the second intercostal space on the right; the tone of the valves of the pulmonary trunk - in the second intercostal space to the left of the sternum.
X-ray anatomy of the heart. X-ray examination of the heart of a living person is carried out mainly by fluoroscopy of the chest in its various positions. Thanks to this, it is possible to examine the heart from all sides and get an idea of its shape, size and position, as well as the state of its sections (ventricles and atria) and the large vessels associated with them (aorta, pulmonary artery, vena cava).
The main position for the study is the anterior position of the subject (the path of the rays is sagittal, dorsoventral). In this position, two light pulmonary fields are visible, between which there is an intense dark, so-called median, shadow. It is formed by overlapping shadows of the thoracic spine and sternum and the heart, large vessels and organs of the posterior mediastinum between them. However, this middle shadow is considered only as a silhouette of the heart and large vessels, because the rest of the mentioned formations (spine, sternum, etc.) usually do not appear within the cardiovascular shadow. The latter, in normal cases, both on the right and on the left, extends beyond the edges of the spinal column and sternum, which become visible in the anterior position only in pathological cases (curvature of the spine, displacement of the cardiovascular shadow, etc.).
The named middle shadow has the form of a wide strip in the upper part, which expands downward and to the left in the form of an irregular triangle with the base turned downward. The lateral contours of this shadow are in the form of protrusions separated from each other by depressions. These protrusions are called arcs. They correspond to those parts of the heart and the large vessels associated with it, which form the edges of the cardiovascular silhouette.
In the anterior position, the lateral contours of the cardiovascular shadow have two arcs on the right and four on the left. On the right contour, the inferior arch is well grown, which corresponds to the right atrium; the upper weakly convex arch is located medial to the lower one and is formed by the ascending part of the aorta and the superior vena cava. This arch is called vascular. Above the vascular arch, a small arch is still visible, heading up and outward, to the clavicle; it corresponds to the brachiocephalic vein. At the bottom, the arc of the right atrium forms an acute angle with the diaphragm. In this corner, with a low position of the diaphragm at the height of a deep inspiration, it is possible to see a vertical shadow strip, which corresponds to the inferior vena cava.
On the left contour, the uppermost (first) arch corresponds to the arch and the beginning of the descending part of the aorta, the second to the pulmonary trunk, the third to the left ear, and the fourth to the left ventricle. The left atrium, located for the most part on the posterior surface, is not edge-forming during the dorsoventral path of the rays and therefore is not visible in the anterior position. For the same reason, the right ventricle located on the anterior surface is not contoured, which, moreover, merges with the shadow of the liver and diaphragm below. The place of transition of the left ventricular arc to the lower contour of the cardiac silhouette is marked radiographically as the apex of the heart.
In the area of the second and third arcs, the left contour of the heart silhouette has a character of depression or interception, which is called the "waist" of the heart. The latter, as it were, separates the heart itself from the vessels associated with it, which make up the so-called vascular bundle.
By turning the subject around the vertical axis, it is possible to see in oblique positions those segments that are not visible in the anterior position (right ventricle, left atrium, most of the left ventricle). The most widely used are the so-called first (right nipple) and second (left nipple) oblique positions.
When examining in the left nipple position (the subject stands obliquely, adjoining the screen with the area of the left nipple), four pulmonary fields are visible, separated from each other by the sternum by the cardiovascular shadow and the spinal column: above the ascending part of the aorta, then the left atrium and below - the right atrium and the inferior vena cava; the anterior contour of the ascending part of the aorta, the pulmonary trunk and the left ventricle.
- Mitral (mitralis; anat.valva mitralis mitral valve, from the Greek mitra mitra, headdress) - referring to the atrioventricular (mitral) valve of the heart ...
- Chest 1 (thorax, pectus, PNA, BNA, JNA) - the upper part of the body, the border of which is drawn from above from the jugular notch of the sternum along the clavicles and from the acromioclavicular joints to the apex of the spinous process of the VII cervical vertebra, and below from the xiphoid process of the sternum .. ...
News about The diagram of the projection of the heart valves on the anterior chest wall and the main points of listening to heart murmurs
- Vladimir Ivanovich Makolkin Corresponding member RAMS, professor, head. Department of Internal Diseases of the 1st Faculty of Medicine, Moscow Medical Academy. THEM. Sechenova As you know, among the causes of chronic heart failure (CHF), ischemic heart disease (CHD) takes the leading place, while
- Despite antibiotic treatment and the success of heart surgery, infective endocarditis remains a serious, potentially fatal pathology, the frequency of which may increase due to improved survival of patients with congenital cardiopathies. The frequency is 1.35 cases per 1000 per
Discussion Scheme of the projection of the heart valves on the anterior chest wall and the main points of listening to heart murmurs
- 2 years ago I did an ECHOKG. Discovered mitral valve prolapse 3, 5 mm 1 st. , MR 1st, TR1st. Open oval window. And the erratic flow from left to right. A year ago she gave birth and is now worried about palpitations and tachycardia. Today I did another echocardiogram. Aorta - 3.0 cm Left atrium - 2.8 cm Sex
- Dear Doctor! On the issue of mitral valve prolapse in a 12-year-old boy, I am sending the examination results: ECHO-CG study: Project of the aortic root - 21 mm Left atrium - 23 mm Systolic divergence of the leaflets - 13 mm Left ventricle EDC - 43 mm Left ventricle PCB - 28 mm Prezhel
Treatment Scheme of the projection of the heart valves on the anterior chest wall and the main points of listening to heart murmurs
- Any operations for acquired heart defects and coronary artery disease are performed
They do not always coincide with the anatomical localization of their sources - the valves and the holes they close (Fig. 45). So, the mitral valve is projected at the place of attachment of the third rib to the sternum on the left; aortic - in the middle of the sternum at the level of III costal cartilage; pulmonary artery - in the II intercostal space on the left at the edge of the sternum; tricuspid valve - in the middle of the line connecting the attachment points to the sternum of the cartilage III of the left and V of the right ribs. Such proximity of the valve openings to each other makes it difficult to isolate sound phenomena in the place of their true projection onto the chest. In this regard, the places of the best conduction of sound phenomena from each of the valves have been determined.
Rice. 45. Projection of the heart valves on the chest:
A - aortic;
L - pulmonary artery;
D, T - two- and three-leafed.
The place of listening to the bicuspid valve (Fig. 46, a) is the area of the apical impulse, that is, the V intercostal space at a distance of 1-1.5 cm medially from the left mid-clavicular line; aortic valve - II intercostal space on the right at the edge of the sternum (Fig. 46, b), as well as the 5th point of Botkin - Erb (the place of attachment of the III-IV rib to the left edge of the sternum; Fig. 46, c); pulmonary valve - II intercostal space on the left at the edge of the sternum (Fig. 46, d); tricuspid valve - the lower third of the sternum, at the base of the xiphoid process (Fig. 46, e).

Rice. 46. Listening to heart valves:
a - bivalve in the apex area;
b, c - aortic, respectively, in the II intercostal space on the right and at Botkin's point - Erb;
d - pulmonary valve;
d - tricuspid valve;
e - the order of listening to heart sounds.
Listening is carried out in a certain sequence (Fig. 46, e):
- the area of the apical impulse; II intercostal space on the right at the edge of the sternum;
- II intercostal space on the left at the edge of the sternum;
- the lower third of the sternum (at the base of the xiphoid process);
- Botkin point - Erba.
This sequence is due to the frequency of damage to the valves of the heart.
The order of auscultation of the heart valves:
In practically healthy individuals, when listening to the heart, two tones are usually determined - the first and second, sometimes the third (physiological) and even the fourth.
Normal I and II heart sounds (eng.):
First tone is the sum of the sound phenomena that occur in the heart during systole. Therefore, it is called systolic. It occurs as a result of oscillations of the tense muscle of the ventricles (muscular component), closed cusps of the bicuspid and tricuspid valves (valve component), the walls of the aorta and the pulmonary artery in the initial period of blood flow into them from the ventricles (vascular component), atria during their contraction (atrial component).
Formation and components of the I tone (eng.):
Second tone caused by the collapse and resulting vibrations of the valves of the aorta and pulmonary artery. Its appearance coincides with the onset of diastole. Therefore, it is called diastolic.
II heart tone (eng.):
There is a small pause between the first and second tones (no sound phenomena are heard), and the second tone is followed by a long pause, after which the tone appears again. However, students who begin training often have great difficulty distinguishing between the first and second tones. To facilitate this task, it is recommended to listen to healthy people with slow heart rates first. Normally, the first tone is heard louder at the apex of the heart and in the lower part of the sternum (Fig. 47, a). This is due to the fact that sound phenomena from the mitral valve are better conducted to the apex of the heart and the systolic tension of the left ventricle is more pronounced than that of the right. The second tone is heard louder at the base of the heart (in places where the aorta and pulmonary artery are auscultated; Fig. 47, b). The first tone is longer and lower than the second.
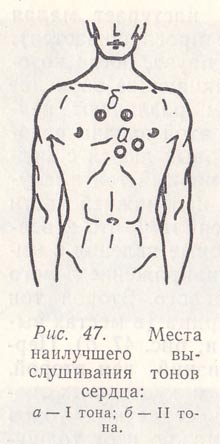
Rice. 47. Places of the best listening to heart sounds:
a - I tone;
b - II tone.
Listening alternately to obese and thin people, one can make sure that the volume of heart sounds depends not only on the state of the heart, but also on the thickness of the surrounding tissues. The thicker the muscle or fat layer, the lower the volume of the tones, both the first and the second.

Rice. 48. Determination of the I heart sound by the apical impulse (a) and by the pulse of the carotid artery (b).
Heart sounds should be learned to differentiate not only by the relative loudness at the apex and base of it, by their different duration and timbre, but also by the coincidence of the appearance of the first tone and pulse on the carotid artery or the first tone and apical impulse (Fig. 48). It is impossible to navigate by the pulse on the radial artery, since it appears later than the first tone, especially with a frequent rhythm. It is important to distinguish between the first and second tones not only in connection with their independent diagnostic significance, but also because they play the role of sound cues for determining noise.
Third tone caused by vibrations of the walls of the ventricles, mainly the left (with rapid filling with blood at the beginning of diastole). It is heard with direct auscultation at the apex of the heart or somewhat inwardly from it, and it is better in the patient's lying position. This tone is very quiet and may not be picked up in the absence of sufficient auscultation experience. It is better heard in young people (in most cases near the apical impulse).
III heart tone (eng.):
Fourth tone is the result of vibrations of the walls of the ventricles during their rapid filling at the end of diastole due to atrial contraction. Heard rarely.
IV heart tone (eng.):
You can listen to heart sounds and murmurs in normal and pathological conditions on the website
Heart valve projections
The right border of the heart is formed by the right surface of the superior vena cava and the edge of the right atrium. It runs from the upper edge of the cartilage of the right II rib at the place of its attachment to the sternum to the upper edge of the cartilage of the III rib 1.0-1.5 cm outward from the right edge of the sternum. Then the right border of the heart, corresponding to the edge of the right atrium, runs arcuate from ribs III to V at a distance of 1-2 cm from the right edge of the sternum.
At the level of V ribs, the right border of the heart passes into the lower border of the heart, which is formed by the edges of the right and partially left ventricles. The lower border runs along an oblique line down and to the left, crosses the sternum over the base of the xiphoid process, then goes to the sixth intercostal space on the left and through the cartilage of the VI rib into the fifth intercostal space, not reaching the mid-clavicular line by 1--2 cm.The apex is projected here hearts.
The left border of the heart is made up of the aortic arch, pulmonary trunk, left ear and left ventricle. From the apex of the heart, it runs in a convex outward arc to the lower edge of the III rib 2-2.5 cm to the left of the edge of the sternum. At the level of the third rib, it corresponds to the left ear. Rising upward, at the level of the second intercostal space, it corresponds to the projection of the pulmonary trunk. At the level of the upper edge of the II rib, 2 cm to the left of the edge of the sternum, it corresponds to the projection of the aortic arch and rises to the lower edge of the I rib at the place of its attachment to the sternum on the left.
The ventricular outlets (into the aorta and pulmonary trunk) lie at level III of the left costal cartilage, the pulmonary trunk (ostium trunci pulmonalis) - at the sternal end of this cartilage, the aorta (ostium aortae) - behind the sternum somewhat to the right.
Both ostia atrioventricularia are projected on a straight line running along the sternum from the third left to the fifth right intercostal space - the left at the left edge of the sternum, the right - behind the right half of the sternum.
Anesthesia in patients with acquired lesions of the heart valves and pericardium
It is characterized by the presence of constant forced filling of the left ventricle in diastole not only from the left atrium, but also due to reverse blood flow (regurgitation) through incompetent aortic valves ...
Innervation of the heart
The activity of the heart is controlled by the heart centers of the medulla oblongata and the pons pons. Impulses from the heart centers are transmitted along sympathetic nerves and parasympathetic nerves, they relate to the frequency of contractions ...
Providing emergency medical care
The main resuscitation measures also include heart massage, which is a rhythmic compression of the heart, carried out in order to restore its activity and maintain blood circulation in the body ...
Essays on Medicine
HDS - the work of the heart with a high power of the blood flow (BMD> 0.93 W), which leads to its hypertrophy and dilatation with subsequent heart failure (variants with cardiac hyperdynamic, Table 3.2). GDS reasons: excessive physical activity ...
Heart damage from chest trauma
Aortic valve rupture is the most common valvular injury in patients with non-penetrating trauma to the heart ...
Chest damage
Refers to the number of extremely dangerous injuries. Extensive injuries result in immediate death. About 15% of victims with stab and small cut wounds to the heart can live for some time even in the absence of help. They are dying ...
Artificial heart valves There are currently two main types of artificial heart valves: mechanical and biological, which have their own characteristics, advantages and disadvantages ...
Development of technology for producing composite materials based on fluoroplastic and fluorinated rubber for cardiovascular surgery
There are three types of mechanical heart valves - ball, oblique disc and bicuspid - in various modifications. The first artificial heart valve was a ball, it consists of a metal frame ...
Development of technology for producing composite materials based on fluoroplastic and fluorinated rubber for cardiovascular surgery
Biocompatibility is the ability of a material to act, causing an adequate response from the body in each specific case of its use. Biomaterials used for the manufacture of prosthetic heart valves ...
Calculation of statistical characteristics of human RR-interval sequences
To understand the tasks of automatic analysis of an electrocardiosignal, algorithms for detecting cardiac arrhythmias and the principles of functioning of such a complex device as a cardiac monitor ...
Regulation of cardiac activity
The heart is a richly innervated organ. A large number of receptors located in the walls of the heart chambers and in the epicardium, allows us to speak of it as a reflexogenic zone ...
The cardiovascular system
The heart is located in the rib cage behind the sternum and in front of the descending aortic arch and esophagus. It is attached to the central ligament of the diaphragm muscle. There is one lung on both sides ...
The structure of the cardiovascular system, gustatory organ, assessment of the feet for the presence of flat feet
As you know, the heart is able to contract or work outside the body, i.e. in isolation. True, it can do it for a short time ...
Chronic obstructive pulmonary disease
ECG from 12/16/2013 - Sinus tachycardia - Supraventricular extrasystole with aberrant conduction - Right atrial hypertrophy in holes. II AVF P wave acute - Right ventricular hypertrophy Spirography and reversibility test from 16.02 ...
Electrocardiograph. Electrophysiological instrumental diagnostics
The electrical axis of the heart is the projection of the resulting vector of ventricular excitation in the frontal plane (projection onto the I axis of the standard electrocardiographic lead) ...
Choosing men's sunglasses correctly
Raw bread with sprouts, flaxseed and vegetables
From what they drink the mummy. Application of mumiyo. Respiratory diseases
Rejuvenating and cleansing detox program at home Body cleansing program for a week
How to get rid of crow's feet around the eyes: the best methods at home